Not surprisingly, the healthcare reform debate has taken many twists and turns since the last real attempt at overhaul in 1993. With more than 45 million people uninsured, and tens of millions more underinsured, the recent focus on universal coverage is not only laudable, but essential. The efforts of longstanding universal coverage advocates were instrumental in achieving this and deserve our continued support. In particular, in this forum, nyceve, California Nurses Association, and many others who make up the Netroots Nation have passionately and sensitively 1) highlighted the moral outrage and disturbing injustice of how the insured and insured alike are dealt with by insurance companies and our health care system and 2) translated this understanding into concrete advocacy and action.
Advocating for universal coverage, however, is not enough. More below the fold.
The attention paid to universal coverage by our presidential candidates and to ‘single payer’ as almost a panacea by regular diarists/commentators in this forum has obscured other very significant problems of our health care system. In this diary (hopefully a first in a series, if it is appreciated), I will argue that in this "political/policy window of opportunity" to achieve real change in how health care is delivered in the U.S., we in the Netroots Nation and others must demand comprehensive reform that addresses other key challenges as well. Anything less will be akin to bringing the uninsured (who currently quite unethically languish without care) onto an already sinking ship on which there are already hundreds of thousands of unnecessary casualties. With the growing influence of Netroots and our unique ability to inject sophistication and nuance into policy debate, it is incumbent on us to agitate for as much real reform as we can get. As we all know, opportunities for transformative policy change seldom come often.
Before I proceed with my argument, I feel compelled to provide some personal background (much to my surprise, comments I made along these lines in a diary a few days ago were met with suspicions (and arguably, accusations) that such arguments are "republican talking points" and that those making them must be "trolls" or "spies"). So, in the interest of full disclosure, I am a physician and a researcher. I practice and teach at one of the top medical schools in the country, and I do research on health policy and disparities in health and publish my work in peer-reviewed medical journals. As my primary appointment is in research, my compensation is derived from the University as well as NIH and foundation grant support. I am not compensated by insurance company reimbursement. I consider myself progressive and am a member of the National Physician’s Alliance.
For the purposes of this diary, I’d like to break down healthcare reform components into 3 broad and essential categories: access, cost, and quality.
Access
Access to healthcare is generally the first thing we progressives think of when considering reform. That universal coverage is necessary from an ethical and efficiency point of view is, I believe, widely accepted in this forum. As nyceve and others have pointed out so well, we must do all that we can to ensure that the rhetoric and proposals for achieving this goal are reached by the political process. Where the issue becomes more confusing, of course, is how exactly to get there. But let’s leave that aside for other diaries so that we can highlight the 2 other reform issues that should not be neglected – cost & quality.
Cost
That health care costs (to the patient, the system, etc) are rising at an unsustainable pace is I think widely accepted. There has been a lot of discussion on this site about the potential for a single payer system to achieve dramatic reductions in costs of health care by reducing the administrative waste of insurance companies. Based on study published in the New England Journal of Medicine by Steffie Woolhandler and colleagues, an often quoted statistic is 31% of costs would be saved if we got rid of the insurance companies. 31% is probably an overstatement since Woolhandler’s article reports that 31% of all U.S. spending is on administrative costs compared to 16% in Canada where a predominantly single payer system exists – i.e. there will be at least some nontrivial administrative costs even with single payer. Even still, let’s say that we could reduce costs by 20% if we cut out insurance companies and have the government (or some quasi-government agency) pay for services, that would mean a huge freeing up of resources that could be dedicated to providing services to the population. This would be a great step forward for reform.
I would argue, though, these resources will not nearly be sufficient to meet the demand for appropriate and equitable health care services without also 1) reforming the way physicians are paid for services, 2) refocusing priorities on preventative health and health promotion, 3) improving quality of care, 4) and developing a publicly acceptable policy of determining how best as a society we can judiciously use increasingly expensive medical technologies and interventions. For the remainder of the diary, I’d like to focus on #3 and leave the others for another diary/another day. I will provide 2 recent popular press links that relate to #1and #4.
Here is what I think are some useful illustrations of the cost problem:
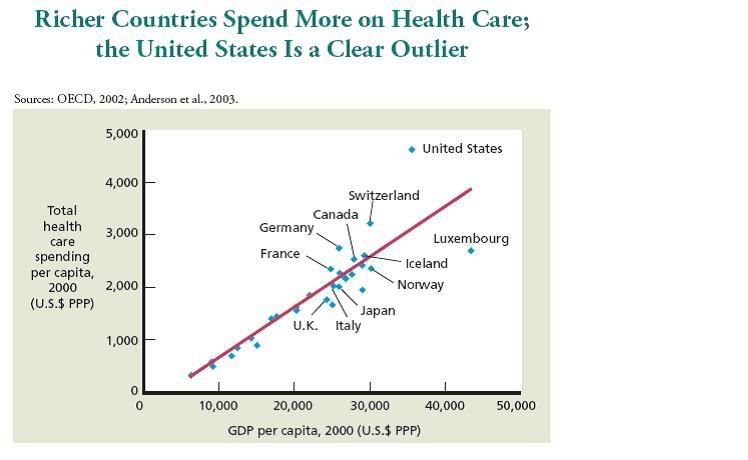
Here, we can see, as countries become richer, they spend more per capita on health care. The U.S., of course, is a clear outlier, spending far more per capita than expected based on our per capita GDP, and yet, as well know, ranking quite poorly on most health care performance indices.
The next graph, though, I think is crucial to my point about rising costs, regardless of the type of system you have:
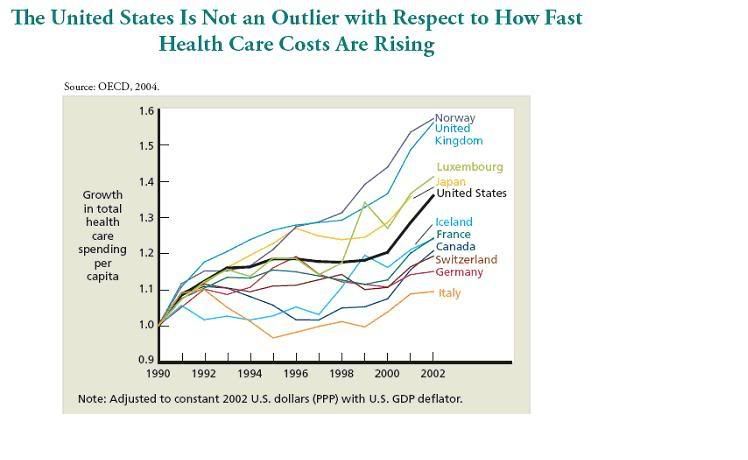
So, by the very nature of increasing longevity, burdens of chronic illness in resource-rich countries, and advancement in medical technologies that not only bring longer life but also very expensive interventions, we can see that regardless of the type of health care system you have (single payer or privately funded), health care costs are growing at a pace that would arguably leave precious little resources left over for other public goods like education, infrastructure, scientific research, and the arts.
Here is one last exhibit indicating why costs are rising so fast – questionable use of medical technology.
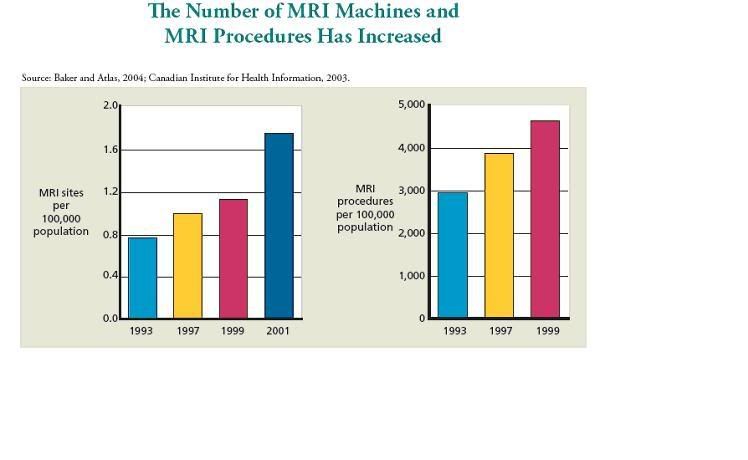
This is the ‘if you build it, they will come’ phenomenon. From 1993 to 1999, we went from about 3000 MRI procedures to more 4500 procedures per 100,000 Americans. Demand for these procedures was created by the growing supply of MRI centers (and the need to use them to recoup costs of building them) and the fact that physicians are incentivized by most systems to justify ordering such tests, even when perhaps unnecessary. Did some people in 1999 get MRI procedures that tangibly helped the physician in the care of the patient who wouldn’t have otherwise in 1993 – absolutely. However, did a significant number of people in 1999 also get MRIs they probably didn’t need and that wasn’t medically indicated – also, yes.
There are number of proposals, like reforming the way physicians are paid etc, that attempt to address the rising cost problem. Given the length of this already, I will leave these for another time.
Quality
If we focus on people who actually do have access to health care (reasonably insured populations), we find a breathtakingly poor track record in quality of care delivered– a track record that would never be tolerated in other industries where lives are at stake – like commercial aviation for example. The reasons for poor quality are multiple and systemic, and should not implicate physicians alone.
Here are the dimensions of quality I’m referring to, as defined by the Institute of Medicine:
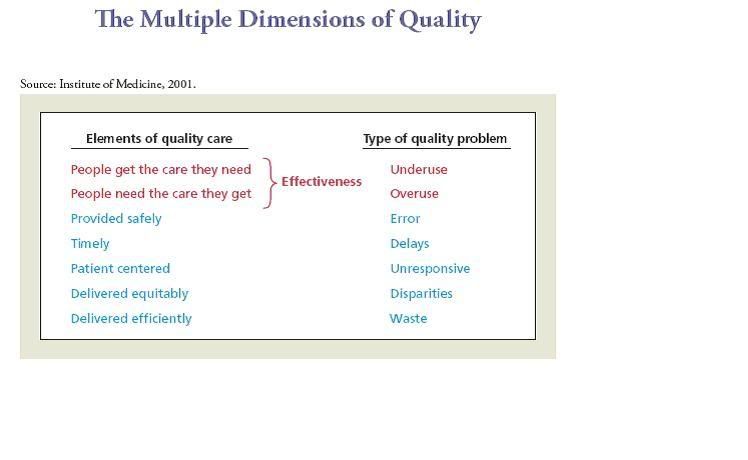
People should get the care they need; when they don’t, we call it underuse. This problem occurs when health care interventions that are known to improve people’s health are not provided to those who could benefit.
People should need the care they receive; when they don’t, we call it overuse. This problem occurs when people receive health care interventions that are not expected to improve their health or may even be harmful.
Care should be provided safely. When it isn’t, we refer to the problem as medical error. Care should be provided in a timely manner, which means that patients do not experience unreasonable or unacceptable delays. Care should be patient centered. When it isn’t, patients experience the health care system as unresponsive to their needs and preferences. Care should be delivered equitably. When it isn’t, we observe differences in who receives appropriate or effective care that are not related to health needs. These differences are called disparities. Care should be delivered efficiently. When it isn’t, we find that the health care system is wasting resources.
So how are we doing on quality of care? Here are some exhibits:
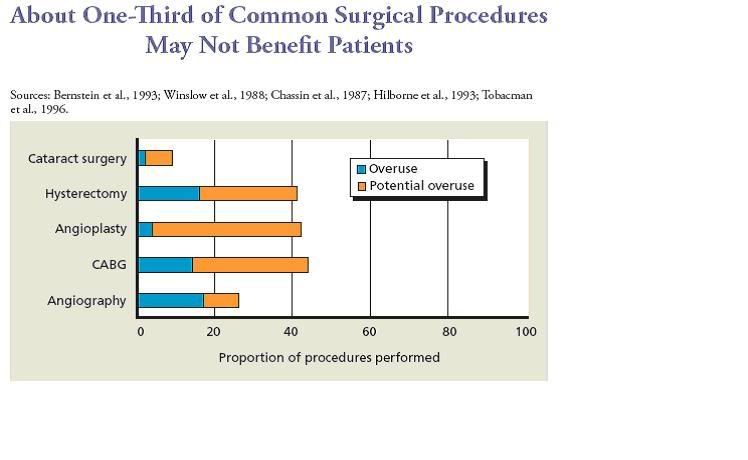
On average, about one-third of procedures were provided for reasons that were not supported by clinical research and may have been harmful to patients.
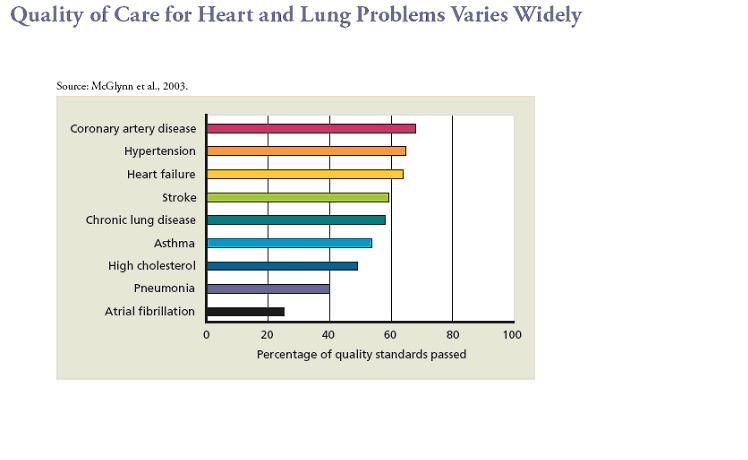
In a national study on quality of care published in the New England Journal, McGlynn and colleagues at RAND found that found that American adults were receiving about one-half (55%) of recommended medical services—that is, services shown in the scientific literature to be effective in specific circumstances and agreed upon by medical experts. This study used a comprehensive method for assessing quality that includes 439 measures of effectiveness for 30 acute and chronic health problems of adults as well as the leading preventive health care interventions.
Here is an example of how quality standards varied by type of medical problem:
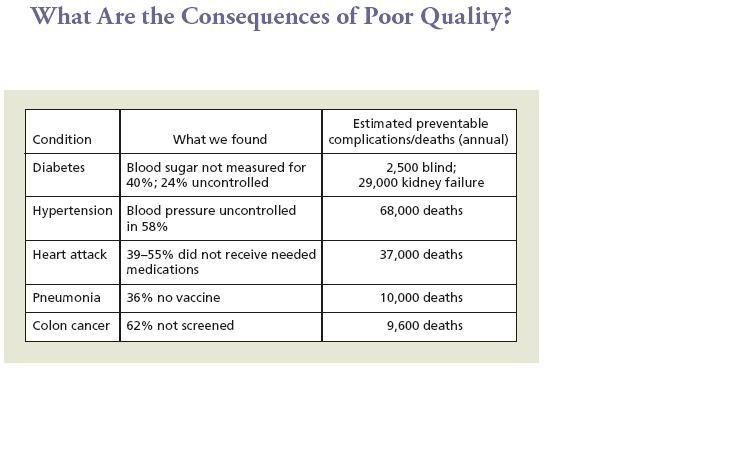
Here is an example of the complications/deaths we can attribute to the poor quality found in the McGlynn study – all of which are preventable if medical care was appropriately provided.
So, the point of all of this was not to depress you, or to paralyze/dilute the excellent advocacy and action on access to care that Kossacks and coalition partners are so gallantly leading. Rather, my goal is to try and push our community here to engage a wider, and as crucial, set of healthcare issues as we approach this most precious opportunity to reform our health care system. Netroots Nation has proven an incredible vehicle for productive advocacy on policy, and what better time than now to begin preparing ourselves for our role in the upcoming health care reform fight.
Note: The graphs posted here are derived from peer reviewed medical journal articles or OECD data and were copied from a RAND Healthdocument prepared by Dana Goldman and Elizabeth McGlynn. The RAND Corporation is a nonprofit research organization providing objective analysis and effective solutions that address the challenges facing the public and private sectors around the world.
