The amphetamines are rather small, simple molecules with enormous pharmacological effects. There are two main divisions of them, at least from a pharmacological viewpoint: the stimulant amphetamines and the psychedelic ones. We shall discuss the stimulant ones this evening and the psychedelic ones when we discuss other psychedelics.
The most commonly encountered amphetamines are amphetamine itself, dextroamphetamine, methamphetamine, and methylphenidate (Ritalin). Ritalin is not strictly an amphetamine, but for most purposes works pretty much the same way.
The amphetamines are chiral compounds, and my diary about chirality is here. The d isomers of amphetamine and methamphetamine have a greater stimulatory activity, but the l isomers have some activity. As we discuss the pharmacological effects we will see where the differences lie.
Here are structural formulae for amphetamine, methamphetamine, and methylphenidate.
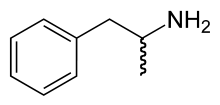
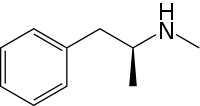
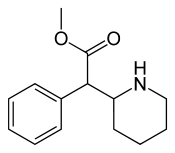
The squiggly line on the formula for amphetamine indicates that the methyl group can either be pointed into your screen (the l one) or out of your screen (the d one). Note that methamphetamine is almost identical except it has an extra methyl group on the nitrogen. Methylphenidate still has the same basic skeleton, with a nitrogen separated from the benzene ring by two carbons. Because of different synthetic methods, amphetamine is synthesized as an 50:50 mixture of the two isomers, whilst methamphetamine is the d one only. We will not discuss syntheses.
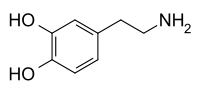
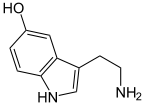
To have some perspective, here are the neurotransmitters norepinepherine, dopamine, and serotonin. Note the close structural similarities between the first two and the amphetamines. Serotonin is not that closely related, but burn that structure into your brain because it will become important when we discuss the psychedelic drugs.

The amphetamines work on several neural pathways. For a primer on the basics, the first installment in this series is here. Amphetamines interact with the dopamine, the serotonin, and the norepinephrine systems. However, it is still not completely know what the exact mechanisms for these interactions are. It is known that amphetamines increase the concentration of dopamine in the space between the pre and postsynaptic neurons, thus triggering the brain's reward system, making it addictive. It is thought that amphetamine both directly causes dopamine to be released and also inhibits the reuptake of it, giving it a double whammy.
It is also known that for methamphetamine at least, and probably for the others, high concentrations are toxic to some of the dopamine producing neurons. Thus, long term, high dose amphetamine abuse can cause irreversible changes in the brain, making complete recovery unlikely although it is possible to quit the drug.
Reuptake of norepinepherine is blocked by amphetamine, giving rise to the stimulatory properties of the drug. Additionally, serotonin, a mood related neurotransmitter, reuptake is also blocked, leading to the feelings of good mood. The modern antidepressants, such as Prozac, work to inhibit serotonin reuptake, but do not have the euphoria component that amphetamines have. There is also some evidence that glutamate levels are also increased. Glutamate is pretty much the opposite of GABA (see the installment on alcohol here), in that it is an excitatory neurotransmitter rather than an inhibitory one. Thus, amphetamines have multiple actions, the sum of which cause the effects and addiction potential.
Methamphetamine has greater effects than amphetamine because not only is the the d isomer, but also because the extra methyl group on the nitrogen increases its penetration through the blood brain barrier. Methamphetamine may be the most addictive drug known because of the combination of effects of energy, alertness, mood elevation, and activation of the reward system. Like cocaine, animal studies show that test animals will literally starve themselves to death when given the choice of a food lever and a drug lever. It does not take long, either.
There are legitimate medical uses for amphetamines, and they are in Schedule II. Uses include attention deficit hyperactivity disorder (ADHD), mostly in children, and the rare condition narcolepsy, where people suddenly fall asleep while doing everyday tasks. It seems paradoxical at first that a stimulant would calm down a hyperactive child, but the logic is that the increased ability to concentrate allows the patient to focus on the task at hand rather than go from thought to thought.
Historically, amphetamines have been used for two main reasons: to increase alertness whilst performing tasks requiring long hours, such as long haul trucking and cramming for examinations, and for appetite control. Used short term, they can be very effective for these uses, but because the abuse potential is so high no physician in her or his right mind would prescribe them for this like that any more. Some of the less potent derivatives are still used for appetite control, but after the phenphen debacle other methods for weight control are gaining favor.
The military has long been a major user of amphetamines. Soldiers on long marches, pilots on long missions, and others were given them to stay alert and keep awake. Current information is hard to come by for military uses, but it is safe to assume that they are still being used in these arenas. During World War II, the Axis powers gave large doses to tank crews, for example, to increase aggression and boldness. Kamikaze pilots were given large doses to produce fearlessness.
Methamphetamine abuse is pretty much epidemic in the United States, particularly in rural areas. Originally a west coast phenomenon (the Hell's Angels were big into it in the 1970s), it has spread nationwide. By the way, I think that the street name "crank" did not come from the Angels carrying it in the crankcases of the bikes. The heat would degrade it regardless of how well sealed a package could be made. Because of the relative ease in manufacture and availability of starting materials, clandestine laboratories are common, but not as widespread as a few years ago. Most illegal methamphetamine is made by huge illegal laboratories and delivered to dealers.
Part of the reason for the drop in small laboratories is the difficulty in getting significant amounts of ephedrine or pseudoephedrine, the essential starting materials for most all syntheses. Federal and state law has really tightened up now. Recently, Mrs. Translator had bad nasal congestion and asked me to go to the pharmacy and get some pseudoephedrine for her. It took nearly half an hour for them to enter my drivers license information and get an answer back from the database that showed that I could buy it, and to log the purchase into the database. In Arkansas, and many other states, every purchase is tracked and entered into the database. If you try to buy more than the allotment, you are committing a crime.
Amphetamine itself is a liquid, and used to be put in nasal inhalers to relieve stuffy noses. It worked well, but people soon learned to pull the cotton out of the inhaler and taking it instead. Inhalers no longer contain amphetamine. Methamphetamine is a solid. Both of them are often converted to the sulfate salts, all of which are solids. Tablet forms are the sulfate.
So, how is amphetamine abused? We shall focus on methamphetamine now, since it is more commonly encountered than amphetamine in illegal arenas.
Ingestion of the free base or the sulfate is probably still the most common method. It is also the slowest route of absorption and produces the mildest "high". Since rate of absorption is strongly correlated to the intensity of the high, this is not surprising.
Snuffing ("snorting") the sulfate is another route, and is a quicker method of absorption. It also damages the lining of the nose, like any other irritant.
Smoking the free base is one of the most rapid routes of absorption. The high is almost instant and is intense, and it lasts a long time.
Finally, injection of the sulfate is probably the most rapid route of absorption. The entire dose is absorbed in only a few seconds, and the reports from users describe sensations akin to orgasm, but lasting longer.
I try not to be overly critical of people who use drugs, but in the case of methamphetamine I will make an exception. This is a really, really dangerous drug. Addiction can develop rapidly, and tolerance to the drug also develops rapidly, making the abuser want more drug, more often. Unfortunately, tolerance to the damaging physical effects and the neural damage does not occur, just tolerance to the high. The increase in blood pressure is not subject to tolerance, for example.
In addition to the behavioral issues and the other physical issues, there is a curious dental condition associated with methamphetamine use. It is severe decay of multiple teeth simultaneously, with rapid onset and rapid progression. The common name for this condition is meth mouth. I chose not to include a picture of it because it is so horrible looking, but a quick web search will give you all the pictures you can stand.
There are several theories as to what the cause of this condition is, and most authorities agree that it is a combination of factors including decrease in saliva ("cotton mouth"), an unhealthful diet, mainly sugar filled drinks since methamphetamine abusers do not eat very much, and deterioration of personal hygiene. There may be some direct causes as well, but the jury is out on this.
Next time we will discuss cocaine, the other widely used stimulant drug, unless popular demand is otherwise. I am still working on the psychedelic installments, but they are not ready yet. I want to include some cool graphics for those, too.
Well, you have done it again. Another set of perfectly good electrons are now history because of you wasting them on this post. And even though Kos considers becoming a Republican when he reads me say it, I learn much more from posting this series than I could possibly teach doing so.
Warmest regards,
Doc
