I was extremely dismayed Tuesday to read Georgia10's
front pager on the Gallup poll indicating that health care tops the list of American concerns. I wasn't dismayed that Georgia wrote her diary, nor that Americans are worried about health care, but at the Democratic party's
utterly tepid response to the subject. It's a long way down from President Clinton's principled "I'll veto anything that doesn't provide universal coverage" to Mr. Gore's demagoguing of Senator Bradley during the 2000 primaries for attempting the same thing, to where we are now. We need something better. We need Single Payer. And here, just one small click away, is one surgeon's opinion of how we get it.
The party's position, viewed in the best possible light, (a light I had a hard time seeing until I talked to my father and he calmed me down) is "We're going to do a better job of doing the wrong thing." At best, it's rearranging the deck chairs on the
Titanic. From a distance it looks like a health care plan, the same way that from a distance, Frankenstein's monster looks like a person. When you get close, however, you can see where they bolted the head on. The trend should be obvious to anyone who's been following health care policy though.
The biggest failure of the Bush administration's domestic policy is the Medicare Part D(ebacle). It fails for a whole menu of reasons, but in my view its principal shortcoming is its complexity. No one but an expert can understand what is covered, what isn't, when the doughnut hole kicks in, why seniors have to pay retail, what people are "dual eligibles" and how we're supposed to fix it. In a similar way, the health care system as a whole is a mess, and the House Democrats' patchwork quilt approach does nothing of consequence to clean it up.
Before launching in to high wonkery, I want to add some linkage here to a few diaries that have influenced my thinking. First of all, there was Bonddad's "Single Payer: Better, Cheaper, More Competitive", which makes three large points on the subject of Single Payer health care and why it's needed: It costs less, it cuts administrative costs, and it enhances competitiveness for US companies. I'd add a fourth economic impact: A percent of GDP saved in health care spending is a percent of GDP that can be saved or invested or put to some more productive economic purpose. The economist Lester Thurow famously said once that we're not going to get rich by giving each other heart transplants, and it's a point worth making.
Jerome à Paris' remarkable energy diaries inspired me to similar care in getting the numbers right, because we are all members of the reality-based community here. The Energize America - A Blueprint for U.S. Energy Security diary especially stands out because it reaches to come up with a succinct policy position, that could readily be implemented, it seems to me. Thank you from the bottom of the right side of my brain. From the left side, of course, mad props to Maryscott O'Connor and Georgia10, who in different ways remind me of the need for passion, which I forget sometimes in my clinical detachment - a virtue in medicine, but perhaps a handicap in attempting to formulate policy. At YearlyKos, gals, the viognier is on me. Finally, I'd like to thank Marcus Aurelius, who started his meditations this way, and more directly to my mother for introducing me to Aurelius in the first place.
I've been writing diaries on DailyKos for a while now so far this year, and have addressed health care in eight of them. Three had to do with HSAs, but five others had to do with attempting to quantify savings under single payer. If you're interested, feel free to click through. The titles aren't all numbered because I didn't think, at first, that I had that much to say, but the arguments are summarized briefly below.
Specifically:
1: Health Care Costs 1: Why private health care administrative costs are higher identifies the issue with insurer administrative costs - they are incurred whether you deny care or not, which runs up the percentages on the non-patient care side of the equations.
2: Health Care Costs 2: Physicians and hospitals pay also identifies where most of the cost savings really are: in the costs doctors and hospitals incur in order to comply with insurance systems. Overall, the savings in admin costs is over 10% of the total - about 180 billion dollars.
3: Health Care Costs 3: Saving money on prescription drugs compares the various ways prescription drugs are purchased by large HMOs and governments in both the US and Canada, and identifies savings of about 52 billion dollars at a minimum for drug coverage for a single payer system, plus a little extra for savings on durable medical equipment.
4. Health Care Costs 4: Avoidable ER visits and hospitalizations tries to quantify what the savings would be if people who had non-urgent health care needs received primary care in the doctors office rather than the emergency room, and sought it soon enough that the cost of avoidable hospitalizations could be eliminated. The savings would be about 28 billion dollars, which covers approximately a third of the cost of the care of previously uninsured Americans.
5. Health Care Costs 5: Other potential single payer savings lists a few other areas. I found four other possible savings areas here. The elimination of much pharmaceutical company marketing, fraud, increased emphasis on primary care, and a nickel I found under my office sofa accounted for 63 billion dollars and five cents. Pharmaceutical marketing practices are especially expensive and aggressive, and you can read about them in the current issue of The Atlantic (subscription only, but it's on the newsstands now if you want to read it the hard way). The nicest thing a (fellow doctor) blind date ever said to me when I visited his practice was, "Wow! I thought you were the new Pfizer rep!"
Balanced against these savings, you have to stack up the increased costs of care. I decided in doing this that I wasn't going to get into a 1993-style argument about which procedure was going to be covered and just covered everything. I threw it all in - dental, orthodontics, mental health, co-payments, increased utilization from the uninsured, a full raft of services for the underinsured, and a pony. The table follows the pattern and methodology of a study conducted to support the California Single Payer Health Care initiative, though the specific values are generated by me and the reasoning behind them is mine except as referenced. The numbers in the table below are billions and the reference year is 2003, since I didn't have more current numbers conveniently at hand. Following accounting convention, negative numbers are in parentheses.
| Current Health Spending | 1,741 |
| Spending Increases | 201 |
| Covering the Uninsured | 55 |
| Prescription Drugs | 6 |
| Dental Care | 13 |
| Orthodontia | 7 |
| Durable Medical Equipment | 8 |
| Mental Health | 9 |
| Home Health Services | 14 |
| Elimination of Cost Sharing | 90 |
| Spending Reductions | (277) |
| Increased Primary Care Emphasis | (32) |
| Prescription Drugs | (42) |
| Durable Medical Equipment | (7) |
| Insurer Administration | (92) |
| Hospital Administration | (34) |
| Physician Administration | (63) |
| Reduced Fraud | (7) |
| Net Change | (76) |
| AmberJane's "Should Cost" Plan | 1,665 |
I don't see any compelling reason that the numbers couldn't be lower and the savings greater, but I think these numbers are probably accurate to within ten percent or so. Certainly other improvements, particularly in preventive care and prescription drugs, could be harvested but I'm trying to be as non-controversial as possible here because I want to talk about the big problem: How to pay for it.
Currently 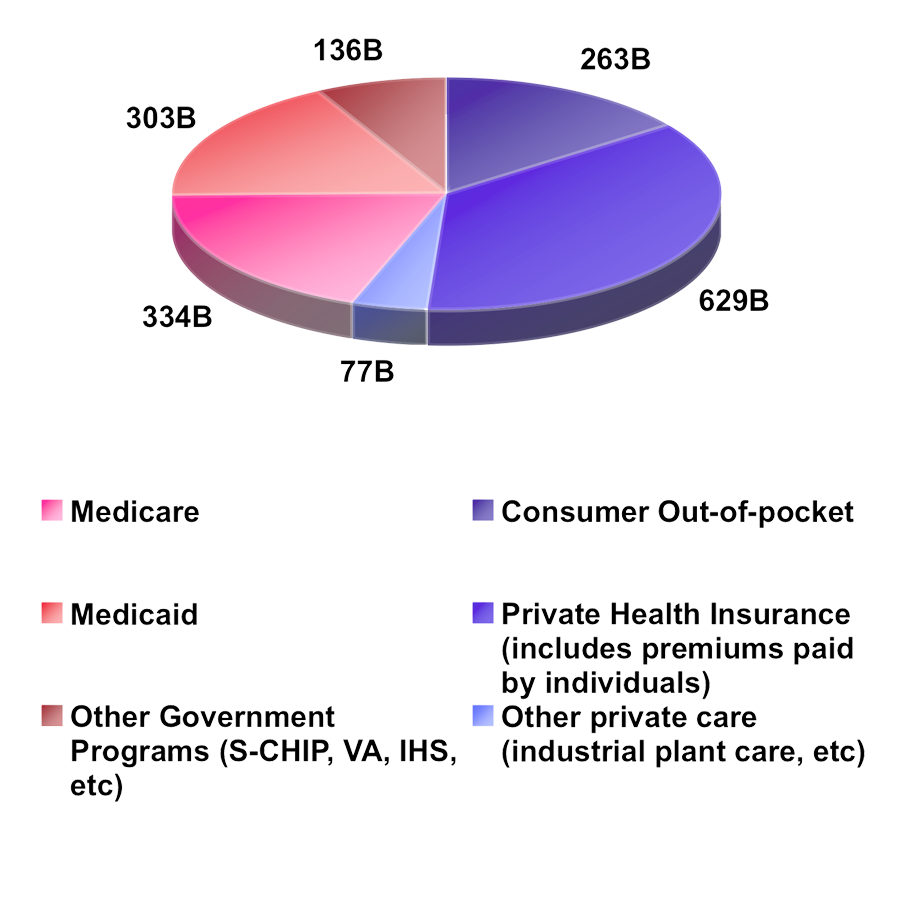 , health care spending comes about 45% from public sources and about 55% from private sources. That's been remarkably consistent over the last decade. I made the graph at the right and put it in my photobucket account if you need a close-up, but the numbers from the Center for Medicare and Medicaid Statistics break down as indicated. Numbers, again, are in billions of 2003 dollars. It's useful to have a quick look at the Kaiser Family Foundation's site where the various trends and indicators in the health care marketplace are discussed, and well-sourced, in considerable detail.
, health care spending comes about 45% from public sources and about 55% from private sources. That's been remarkably consistent over the last decade. I made the graph at the right and put it in my photobucket account if you need a close-up, but the numbers from the Center for Medicare and Medicaid Statistics break down as indicated. Numbers, again, are in billions of 2003 dollars. It's useful to have a quick look at the Kaiser Family Foundation's site where the various trends and indicators in the health care marketplace are discussed, and well-sourced, in considerable detail.
My 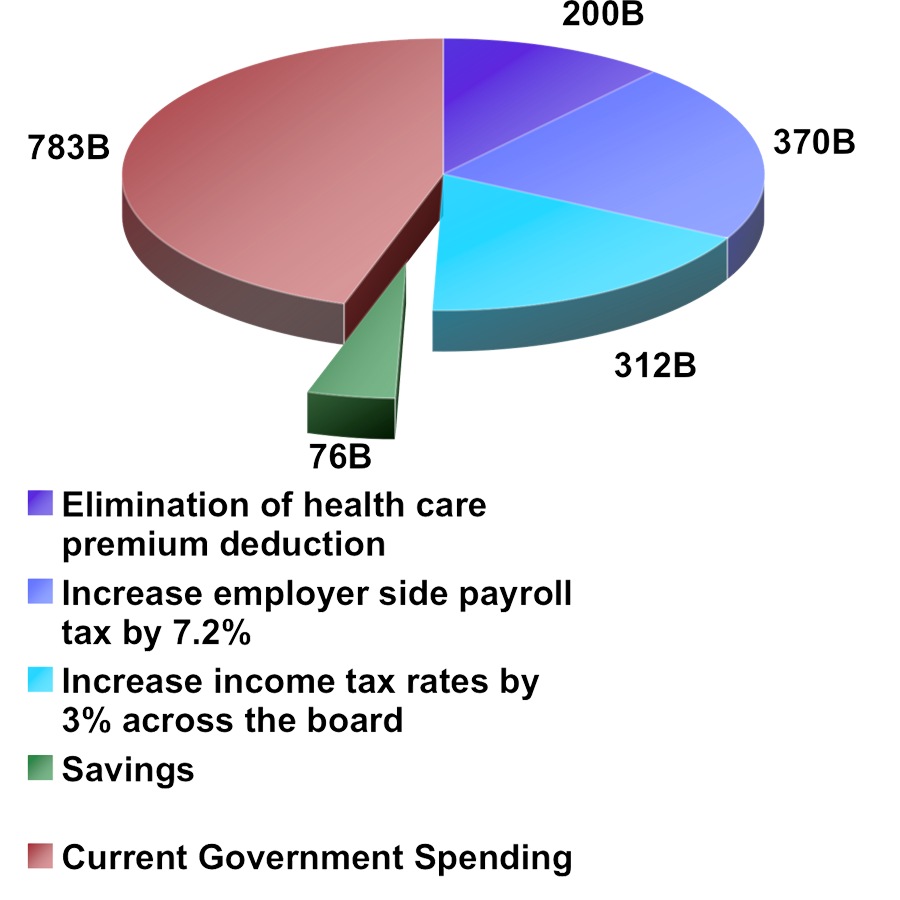 proposal is to continue the 45% of health care spending with revenue streams from current sources. This amounts to about 780 billion dollars. By my reckoning that leaves us about 882 billion dollars short of where we need to be to pay for the plan I outlined. I think we can close the gap in three ways. First, we should eliminate the tax deduction for health insurance premiums. By my estimate, which differs a small amount from the authors of the linked study, there's 200B of potential revenue there. As the removal of a deduction, this is properly classified as money we're already spending on health care, so this should be non-controversial.
proposal is to continue the 45% of health care spending with revenue streams from current sources. This amounts to about 780 billion dollars. By my reckoning that leaves us about 882 billion dollars short of where we need to be to pay for the plan I outlined. I think we can close the gap in three ways. First, we should eliminate the tax deduction for health insurance premiums. By my estimate, which differs a small amount from the authors of the linked study, there's 200B of potential revenue there. As the removal of a deduction, this is properly classified as money we're already spending on health care, so this should be non-controversial.
We still need to come up with another 682 billion dollars, and I propose that this be divided with about 55% from an employer payroll tax and 45% from a personal income tax. The IRS 2004 data book provided much of the data I used here on tax base and current tax revenue. Combined with the Center For Medicare and Medicaid Statistics, I've observed that payroll taxes generate revenue off of a tax base of only about half of the total personal income, since about half the personal income in this country is not from wages. A tax on income will raise about twice the money at the same rate as a tax on payrolls. On the other hand, employers who cover their health care costs out of pretax dollars currently would actually see a net reduction in their costs, since they'd be spending nothing on private insurance any more. You can balance the tax rates between income and payroll tax however you like, but I selected the employer-side payroll tax rate of 7.2% (which would raise 370 billion dollars) and an income tax rate increase for each bracket of 3%, which would raise another 312 billion dollars.
You could add some variations if you really wanted. Every penny of the gas tax is a billion dollars of revenue. The tax on cigarettes could be raised some more I suppose. Rather than an across the board 3% increase in income tax, you could graduate it so that the lower brackets went up a little less and the upper brackets went up a little more, to make it even more progressive. I like the idea of a simple income tax surcharge (something like this is how they pay for health care in Australia), but certainly there's room for debate.
Administration of the new system is also an interesting question. I'd like to see something like the Social Security Administration or the Postal Commission. Make it as apolitical as possible, and leave it to professionals to run. What can't be allowed to happen is administration by political cronies.
Yesterday, Althea in IL posed a pertinent question in her diary. "What is the downside to single payer health care?" Under my plan, which, with a hat tip to DawnG, I'd like to call AmeriCare, the following groups would be worse off:
1. Employers who don't currently provide health care. These are generally relatively low wage operations. The employer side payroll tax I propose, 7.2 percent, gives a cost increase of $3,600 on each employee who makes 50,000 (well above the median wage, by the way). If we're talking about covering everyone, then I think these employers (and I'm looking with cold gray eyes at you, Wal Mart) need to chip in too.
2. For-profit health insurance companies. While some companies can do very well selling Medigap policies, which pay for extras like private rooms that would not necessarily be covered under AmeriCare, there's no question that the health insurance industry would have to move from an underwriting model to a spending-management model, more like dental insurance currently operates. They're smart people; they're up to it. Health care is for people, not profit.
3. Pharmaceutical companies. Marketing costs would be reduced since there's only one customer, but centralized procurement would probably squeeze profits. At the same time, a lot of profit is being sheltered under the practice of writing off free samples at full retail cost rather than production cost against profits, so there's definitely some room to tighten here.
4. Me personally. At the moment, I make a small profit on my health care expenses. That's just silly. Under AmeriCare, my costs would go from a small profit to an increased tax expense of over 35,000 per year. And if a financial hit like that led to universal health care for all Americans, then I would call it a bargain.
Worth every penny.
