We tend to think ourselves as the pinnacles of Creation, high above the other creatures of this planet on the Tree of Life. But if the metric of success is persistence and sheer numbers, the most successful organisms are microbes, some so primitive they aren't even considered
alive. Living or not, from the molecular perspective of these tiny denizens, multicellular new comers like human beings represent only one thing: Fresh meat. Of course, in the aftermath of 9/11 and with the grim spectre of WMDs held over our heads at every opportunity by White House speech writers, we can count on our War President to be on top of a National Disease Emergency, right?
[DR Tara Smith] Despite the lip service paid to making this country "safer" in the aftermath of 9/11, the measures put in place show that protection of our health has become almost exclusively a political issue, and the science is again being ignored.
Tara Smith is one of the frontline warriors in research fighting the ancient scourge of disease in all its forms, from manmade bioterrorism to natural pandemic. I had a chance to ask Tara her expert opinion on the status of that age old threat or how our Federal Government might perform under fire. Her answers are not reassuring ...
Update: For those permalinking in, see
DemFromCT's accompanying post on Government and personal preparedness
DarkSyde (DS): We're just beginning to hear about the significant role that patterns of resistance and susceptibility to disease have played in the rise and fall of rival cultures throughout recorded history. What is a good example of that?
DR Tara Smith (TS): It's amazing just how much microbes have played (and continue to play) a role in our history. The winners and losers in many wars and cultural conflicts have been decided in large part not by brains, battle, or bravery, but by which side had the most participants left standing after being ravaged by one disease or another. This is something that's been known for awhile and is getting further fleshed out with new studies. The best-known example is the introduction of measles and smallpox by Spaniards into the Aztec Indian population (and similar introductions by Westerners into other naïve native populations). It's been estimated that the Indian population in the New World declined 95% in just a few centuries after the arrival of Columbus.
Interestingly, some recent publications have challenged that notion, suggesting instead that it was the re-emergence of a native virus, such as a hantavirus. An interesting idea, but it doesn't explain the spread of population decimation seen in the years following Western contact.
DS: Is bioterrorism or a modern pandemic a real threat to the US?
TS: Well yes, especially as 45 million Americans lack health insurance! This means any outbreak might be essentially invisible to detection until people start reporting to an emergency room with a mysterious illness in enough numbers to stand out. Imagine that they have something serious, such as a multi-drug resistant strain of Mycobacterium tuberculosis. They could have been spreading that for weeks or months, exposing anyone and everyone to a germ that's difficult to treat. Bush's solution to this is Healthcare Spending Accounts; ignoring the fact that health care is a vital issue of national security. The public won't ever be "safe" while so many of us are vulnerable to the cracks in our healthcare system, no matter what the vector of infection.
Many molecular biology techniques are becoming easier and cheaper all the time, making pathogens simpler to manipulate. In theory, an airborne, multidrug resistant bacterium could be created and disseminated via aerosol, creating a huge epidemic. In practice, it's not quite that easy, and a lot of factors need to be taken into account. But we've seen that determined terrorists will often use what they've got, even if it's not especially sophisticated.
While the 2001 anthrax attacks (still unsolved, by the way) certainly got a lot of press, it wasn't the first bioterrorism attack on U.S. soil. Back in 1984, a cult in Oregon sought to influence the outcome of a local election--so they added Salmonella to local salad bars. Extremely low-tech and with an agent not listed on any bioterrorism watch lists, but it sickened around 700 people, so it can be deemed a successful attack.
However, that attack was only recognized retrospectively after a cult member copped to it--a bioterrorism event had taken place essentially under our noses, and no one would have ever found out about it if not for subsequent litigation against the cult members (It was initially blamed on poor food handling practices). This is exactly why so many public health experts scoff when the Bush administration touts how much safer we are. Our public health system is still in a shambles, depleted from years of neglect dating back to the Reagan administration. Better surveillance would help us to detect not only a bioterrorist event, but also an outbreak of a new disease--like "bird flu." As it stands, our surveillance is almost all passive--we rely on health care providers to report their findings to the CDC and other agencies. There's not a lot of coordination--it may take weeks for 2 different states to realize they're both having outbreaks of, say, a gastrointestinal illness. That time lost means additional cases that could have been prevented, especially if the source of the infection is contaminated meat or a similar item that could be sitting in the freezer of thousands of Americans.
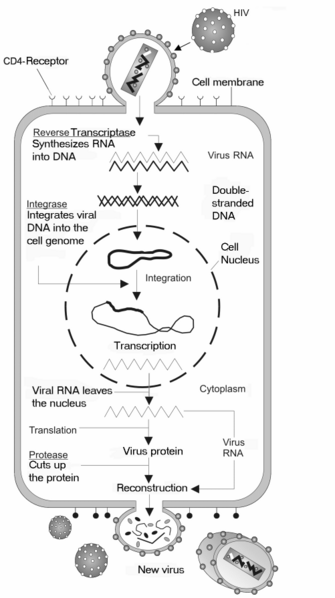
Right: Starting at the top of the illustration, viruses such as influenza and HIV appear like spiky balls or ovoids as they approach their cellular prey. These bugs attach to the cell's membrane and use a process called Receptor Mediated Endocytosis to gain entry to the interior. Essentially, they pick the lock of an existing door in the surface of a cell and walk right in. Middle: Viral elements then take over the nuclear machinery and make more viral packets which head back to the surface where an exit has been constructed. Bottom: The departing new viruses are coated with the cell's own membranous material as they exit the cell and they're on their way to start all over again on another cell. Illustration courtesy Wikipedia
DS: What is Bird Flu as opposed to just 'the flu' and what makes it more dangerous?
TS: "Bird flu" is a highly pathogenic virus of the serotype H5N1 (for an excellent overview of influenza biology, check out the influenza primers on the flu wiki).
To oversimplify a complicated story, the influenza virus genome is composed of 8 segments--the H and N genes compose 2 of these. Influenza viruses can evolve in 2 ways: they can swap these segments to create new combinations (excellent pictorial of that process here), or they can accumulate mutations in the individual genes to create proteins with novel specificities. The latter is what has been happening with H5N1.
From the beginning, H5N1 was a worrisome virus. It has a high mortality rate, it kills quickly, and the young and the healthy--groups which are generally pretty safe from severe influenza symptoms--are targets. It's been found to cause a Cytokine Storm--similar to the 1918 "Spanish" flu virus, that killed 50-100 million people worldwide. This "storm" causes massive inflammation, which can damage lung tissue. Victims can literally drown due to the production of fluid in the lungs. It's not a pretty picture.
H5N1 was first found to infect humans in Hong Kong in 1997, sickening 18; 6 of them died. It infected a number of chickens as well, and was so serious (and bloody) that they nicknamed it "chicken Ebola." Then--it vanished. It came back in 2002, again in Hong Kong, but only in birds at that time. In 2003, it caused more human cases in Hong Kong, and was found in birds throughout Asia. In 2004, the shit really started to hit the fan. Massive poultry die-offs in a number of countries (followed by culling in an effort to stem the spread of infection), and sporadic human cases. These worsened in the last year or so, and they've also caused strange symptoms not often seen with influenza. It presented as a diarrheal illness in 2 children from Vietnam. It's infected tigers, leopards, and domestic house cats--species which are generally not infected by influenza. It's deadly to mice in a lab setting--again, a rarity. Additionally, when the genomic sequence has been examined, it has several mutations that were also seen in the 1918 influenza virus. It's just a strange, nasty virus, and human cases are being found in new areas every month. Humans have died from it in Indonesia, Vietnam, China, Cambodia, Turkey, and now apparently Iraq, and it has been found in birds in a number of additional countries. So far, no human-to-human (H2H) transmission has been confirmed, but this is suspected in several cases. That H2H transmission will become a widespread mode of spread is the biggest fear of those of us in public health keeping an eye on the situation.
DS: What can people do to protect themselves? Is a vaccine available?
TS: There is not yet an effective vaccine that's widely available, although several groups are working on developing one. It's a challenging task. Influenza vaccines have long been made in eggs, but this particular virus is lethal to eggs. Therefore, the virus has to be manipulated so that it doesn't kill the very biologic factory we use for production.
Scientists are working on other ways to develop and manufacture these vaccines. One possibility is to use DNA vaccination. Using this method, DNA encoding viral genes are injected into the muscle. Our own cells then produce viral proteins, which are recognized by the immune system as foreign. An advantage of this is that these vaccines can be made quickly, so we can carefully match them to the virus that is circulating, eliminating the need for stockpiling. The downside is that these haven't been very effective yet in tests. Still, we need these kinds of novel ideas to get away from the egg-based (or even tissue culture-based, where they use cultured cells in a Petri dish) technologies.
As far as what individuals can do, right now, the best advice is simple hygiene. Wash your hands, and avoid touching your eyes, nose, and mouth. Don't spread your own germs to others--stay home if you're ill. Get a flu shot. It won't protect you from "bird flu," but remember that 36,000 people die every year in the U.S. from garden-variety influenza. Additionally, fewer people incubating currently circulating human strains means less chance for H5N1 to meet up with these viruses and potentially swap genes.
Additionally, in the event of a pandemic, many basic services likely will not be up and running. It's a good idea to have a stock of food, water, medications and basic necessities in the event of any emergency--influenza is only one such natural disaster that could result in you being unable to make it to the grocery store.
DS: In your opinion, what grade would the Federal Gov get as far as being able to create, distribute, and administer treatment to enough people in the event of a Bird Flu pandemic?
TS: Right now, we're failing. For instance, at the start of the 1990s, there were 5 manufacturers of injected influenza vaccine in the US. Now we have 2. No significant new technologies have been developed to improve influenza virus manufacture in many decades; we're using an antiquated process. As I mentioned, other techniques are being investigated, but none are ready to go. So, we're stuck with the egg procedure for the time being. As far as distribution and administration, things aren't much better. Homeland Security is now in charge of much of this, and as Katrina showed, we have real communication and chain-of-command problems. These need to be resolved before something like this could succeed.
It's not hopeless--we've distributed vaccine to entire cities in a matter of days in Africa, and eradicated smallpox world-wide in a decade of intense vaccination. But right now, we're simply not ready.
DS: Is evolutionary biology a component of the science underlying your field, and if so can you give an example?
TS: Absolutely. The influenza virus is an RNA virus, and can easily mutate. This leads to slightly different viruses each year--meaning the vaccine we use must be re-formulated on a yearly basis. Data from influenza surveillance is used in conjunction with the principles of evolutionary biology in order to predict what types of viruses will be most common the following year, so that the vaccine can be produced in time for the influenza season.
This is also a problem for the H5N1 virus. Vaccines are currently being produced that should, in theory, protect us from the virus--but what if it doesn't become widespread for another 5 years? Would a vaccine formulated against the currently circulating H5N1 viruses protect us? Would the changes be too great? Influenza is a moving target--and it evolves rapidly.
It's sadly ironic, though. Most creationists accept this kind of evolution--I wrote a few months ago about an article Casey Luskin of the Discovery Institute wrote, where he discussed influenza virus evolution. He claimed it wasn't a good example of evolution, because after all, "they're still viruses." So they dismiss some of our best examples of evolution in action because it's not as dramatic as seeing a cat turn into a dog, or whatever crazy idea of evolution they espouse. It's enough to drive a biologist nuts.
DS: Speaking of evolution and pseudoscience, I've seen a few articles by folks normally associated with the Intelligent Design Movement, AKA "Bush's Base", who are skeptical about the link between HIV and AIDS. What's that all about? How solid is the link between the two?
TS: The link is about as solid as it gets. There are certainly still gaps in our knowledge, as there are in any area of science. For example, I know you've written previously about a mutation called CCR5 delta 32 that appears to provide resistance to HIV infection, and there are likely other factors that affect the course of disease. Others have looked at the presence of a second virus that, when present, seems to also provide protection from disease progression. So there's a lot of interesting avenues of research, and we don't understand the entire picture. But there's no doubt whatsoever in the mainstream scientific community that HIV is the cause of AIDS.
As far as why advocates of ID and some fundamentalists would deny it, well, I'm sure you've probably seen the Discovery Institute's Wedge document. They make it very clear that they're not so interested in the science--that's just a means to an end, which is winning the "culture war" and turning America into a right-wing theocracy. They started with evolution because ever since Darwin, there have been religious objections to the theory--"my ancestors weren't no monkeys!" and the like. Likewise with AIDS. In the beginning of the epidemic, it was characterized as a "gay plague," and it suits the agenda of some evolution-deniers better if it retains that stigma. AIDS caused by a virus means that almost anyone is potentially at risk. AIDS caused by "lifestyle choices" such as men having sex with men, or the use of a variety of illegal drugs, or prostitution means that it's only those marginalized groups that are at risk--and good right-wing fundamentalists like Phillip Johnson and Jonathan Wells of the Discovery Institute can point to the "immorality" of victims as the cause of their illness.
It's not only the religious right that denies that HIV causes AIDS, however. This is a meme that's increasingly being advocated by traditionally progressive groups. For example, the ACT-UP ("AIDS coalition to unleash power") group in San Francisco--which used to prominently advocate for HIV education and funding--has now turned around 180º and declares that it's actually HIV-fighting drugs such as AZT that cause AIDS. They're joined by Christine Maggiore and her group Alive and Well. Maggiore herself has been diagnosed as HIV+ but has claimed the diagnosis is meaningless--and she recently lost her 3-year-old daughter, due to infection with Pneumocystis carinii, an infection commonly seen in AIDS patients.
DS: Other forms of "faith-based" or "alternative" medicine also seem to be increasingly funded with taxpayer dollars. What do you think about that?
TS: This is one of the things that got me interested in epidemiology when I was a freshman in high school. My mother has multiple sclerosis, and she was always receiving information about all kinds of "alternative" therapies--chelation, bee sting therapy, vitamin regimens, etc. So I learned young how to investigate claims like these--and generally find them to be empty. In anything faith-based, of course, it's really difficult to study it rigorously; how can you rule out the intervention of a deity? And with various types of alternative healing, there's a lot of post hoc, ergo propter hoc (following, therefore because of) thinking: "I felt so horrible before I started this treatment, and now I feel great. It works!" Placebo can be a powerful thing.
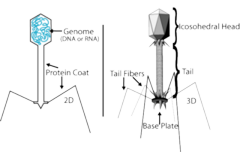 Looking more like a microscopic lunar lander than a microbe, this virus, called a Bacteriophage, lands on the target cell and proceeds to drill right in like an oil rig. Once the hole is made, it then injects the genetic material in the head straight into its victim to carry on the assault. Illustration courtesy of Michael Jones
Looking more like a microscopic lunar lander than a microbe, this virus, called a Bacteriophage, lands on the target cell and proceeds to drill right in like an oil rig. Once the hole is made, it then injects the genetic material in the head straight into its victim to carry on the assault. Illustration courtesy of Michael Jones
DS: How about other potentially harmful outbreaks like Ebola or "flesh-eating" strep; are these still a realistic threat?
TS: Sure. We find out about new diseases almost every day. Some of them show up and seem to fade away, such as SARS. Some surface periodically, causing large but focused outbreaks, as we've seen in recent years from Ebola and Marburg viruses. Others become established, like the West Nile virus. Interestingly, about three-fourths of the new diseases that we've seen over the past few decades have been zoonotic diseases--diseases that are transmitted between animal species. All those I mentioned are examples of this: SARS was found in civet cats and bats, Ebola has now been found in several species of fruit bats (and has also been transmitted to humans from diseased apes), West Nile circulates in birds. And of course, the H5N1 virus is an avian pathogen that has entered our own species. At the Center for Emerging Infectious Diseases here at the University of Iowa, we're building relationships with veterinarians and others who deal with animal health, in order to better deal with these zoonotic diseases. We don't know what Mother Nature is going to throw at us in the future.
Additionally, we're seeing many established pathogens make a resurgence. This could be due to resistance to antibiotics, or due to the acquisition of new virulence factors. Methicillin-resistant Staphylococcus aureus, for instance, has been a scourge in hospitals for many years. Now it's increasingly being found in the community as well. A bacterium called Clostridium difficile--a relative of the bacteria that cause tetanus and botulism--has also been reported to have increased in virulence. And as you mention, Streptococcus pyogenes, or the "flesh-eating" bacterium, has become more dangerous since the 1980s.
It's something that will always be with us--microbes, truly, rule this world, and we'll never "defeat" them. However, we can work to understand them and increase our odds of fighting them to a draw. It's about the best we can hope for.

DR Tara C. Smith blogs on health, infectious disease, and related topics on her blog Aetiology. Tara is an Assistant Professor of Epidemiology in the College of Public Health at the University of Iowa and the deputy director of the university's Center for Emerging Infectious Diseases. Her research involves a number of pathogens at the animal-human nexus. Additionally, she is the founder of Iowa Citizens for Science and a pioneer of the popular science blog The Panda's Thumb

