There was a daughter of a man who took his life too young
she swore she'd never do the same then did just what he'd done.
And there's a boy who's gone insane hears voices in his head
noone knows what they say and no his mother's dead
Audioslave/Exploder
This is not about teabaggers, or republicans or democratic politicians being out of touch with reality.
It's about people who have suffered serious psychiatric illnesses which have destroyed their dreams and taken them far off their intended course in this life.
As you prepare to do Christmas, I want to ask you to think about the things over the jump just a little bit.
If nothing else it will likely help some of you appreciate your families and your health more......and I would be interested in feedback from the Kos community regarding some bright ideas about addressing this systemically - Im fresh out of 'em.
I am a licensed professional counselor and have worked in the field over 25 years primarily with children and families, but in the past 3 years or so, I have made a transition to working with adults with chronic mental illness.
It has been an eye-opening experience, to say the least, I feel I have already learned a lot and I have come across some things that simply chap my hide to no end.
And this story is about how these poor, vulnerable folks get the shaft coming and going and get exploited by the ‘free market dynamics’ that have been unleashed by the privatization of mental health, at least here in Georgia, as well as some glimmers of hope that it won't always be like this. I am certain is it similar in some states. My hope is that it will seem as appalling and outrageous to you as it is to me.
A Vicious Downward Spiral
There is a set of interacting entities and processes or systems which perpetuate their sojourn to the bottom of the socioeconomic ladder and this is why I am interested in ideas about impacting the system that causes this regularity of screwing people who can't afford it.
Historically, mental illness has been very misunderstood and feared and people have developed devastating prejudices about it, along with myths, lies, and false beliefs that persist to this day in some areas.
The whole concept of demon possession and exorcism - as far as I am concerned - is one of the primitive attempts of a primitive people to understand the bizarre occurrences in the lives and actions of people with serious mental illness. I work in Atlanta Georgia I have I have fielded questions about the need for an exorcism as recently as 2 months ago.
I work with people who are my age (50) and those a bit younger and a bit older. To keep a massive topic structured, I am going to focus mainly on people my age.
We all graduated high school about the same time (or dropped out, as is often the case here in Georgia) but whereas I spent my time going to college, getting jobs, working, dating, playing in bands, and trying to keep my act together and eventually buying a home and 'settling down', they have been
· mentally ill: hearing voices, seeing things, deluded by false ideas,
· in and out of hospitals and jails.
· They have experienced pervasive medical neglect and exposure to disease, filth, drugs, crime, and plain old danger.
· They have either lost most of their teeth or they walk around with numerous rotting teeth with abscesses and in need of root canals;
· estranged or alienated from their families
· Homeless - sleeping in abandoned building, under bridges, in alleyways and abandoned houses, on park benches, in the trains to the airport,
· getting charged with loitering, trespassing, sent to jail, released –
Over and over, and over. 24/7/365. They just do not get a break.
They have also been in and out of state hospitals, in sometimes for years or decades. I have met and worked with people older than me who spent 20, 22, 24 years in state hospital, filled with stories of mistreatment and almost always with a shattered self-image from years of being referred to as a schizophrenic or a manic or....a crazy person.
They were bullied and victimized by other patients and by staff people. They spent tears locked away from reality, from society, for the Good life. Then they were discharged to that reality and society that didn't want to deal with them and still, to some extent, hasn't learned how.
A House is not a Home
The myths and ignorance of yesteryear regarding mental illness seems to have encouraged families to 'give up' their mentally-ill member, historically for long-term institutionalization, and others have been consigned to a cycle of homelessness, hospitals, jails, and more and more lately they end up in these usually terrible places called transitional homes..
That link takes you to a google search page for a variety of likely better run places. And there's some good information to be found, but the homes I am talking about aren't really on the map, so to speak.
They have been around for a while but I have only become aware of them in the last 4 or 5 years. For a while I worked in the MR/DD field regularly visiting and monitoring the quality of group/care homes for persons with developmental disabilities (DD). These homes were licensed and under constant scrutiny because - shockingly - people will try to take advantage of the less-fortunate.
People would physically and sexually abuse residents entrusted to them; they would pack 3 times as many people into a home house so they could make lots of money. It was a terrible situation (brought on by the de-institutionalization of MR/DD people). Regulation HAS improved the situation dramatically. Vigilance is essential because people still want to house people just to get the money and drive fancy cars and go on exotic vacations.
In the arena of adult mental health, though, it's a different critter.
I don't know when they began, but I have become aware of these so-called "transitional homes"; a form of 'personal care homes' like those just described for the MR/DD population. There are licenses and unlicensed versions.
I'll start by saying I HAVE seen a couple very good Licensed PCH's that run like you might think they should. They take actual care of the people enrolled with them. They get a real bedroom: sometimes with 1 roommate, often their own room. I think that is an essential part of helping these people achieve some stability. They get 3 meals per day, snacks, they get assistance managing what little money they may have, they will ration their cigarettes to them so the cigarettes will last through the month.
The bulk of them, though, run from terrible to heinous.
The most heinous was in an area of Southwest Atlanta, rife with drugs, crime, and gang activity. The lady who ran the place got it cheap, no doubt, and she herded as many people as she could into this place and charged them each $600 per month.
By the way, these folks get, on average, about $650 - $750 a month in Social Security Disability. Most everybody I have met gets about this much. Some get more but they usually have some serious medical issues, so, despite what the rich-wing wants people to think, SSDI is NOT La Dolce Vita.
In addition to this breathtaking rent, these homes will take ALL the person's food stamps and make them contribute to a communal food arrangement yet will always be running out of food well-before the end of the month. The people are often penniless before the middle of the month, definitely by the latter part of the month, which, of course, is very stressful and exacerbates their condition frequently, causing relapse, return to the hospital, and then discharge back to the home.
Back to the house I was talking about: the lady, in an attempt to not spend any money on utilities, would chain and lock the fridge, turn the gas off so there was no heat, yanked the burners out of the stove so people wouldn't stand around the stove and cook or stay warm. And nailed the back door shut.
She would take all the people's medications and put them in a bag that she kept in her car and dispensed them when she got around to it.
This appears to be connected to the dead person they found in her yard one day about 2 years ago. The cops came, the place was shut very temporarily and was allowed to reopen.
While the dead body is a remarkable exception, the rest of that description is typical of many transitional homes and will probably fail to communicate the travesties that are going on.
Some of the folks I deal with right now tell me stories of 15 and 16 people in a large house, all paying $600 a month and living a very meager existence. There is fighting, stealing, drug use, prostitution, and sheer craziness ongoing day and night. The clients are all different people but the stories are remarkably similar.
Payees
Many of these people, for a variety of reasons, have a "payee", somebody who handles their check and makes money available to them. This is often another obstacle for these people.
A lot of times the payee is unavoidable - people with alcohol and other drug dependence blow their money fast. Many people who are still trying to recover from intense episodes of mental illness will be too confused to be given money.
Payees, of course, will take their money, charge 'fees' that are excessive, will be slow to get things done, be very inconsistent, all of which ADDS to the frustrations of these people already described.
Being an honest sort I think that it has to be possible to set up some sort of secure way to assist these folks in some of their money management. (True - some people are very impulsive with their money'
Maslow's Triangle
Abe Maslow was a psychologist who crafted the theory of the hierarchy of needs
Maslow's hierarchy of needs is often portrayed in the shape of a pyramid, with the largest and most fundamental levels of needs at the bottom, and the need for self-actualization at the top.[1][6]
The most fundamental and basic four layers of the pyramid contain what Maslow called "deficiency needs" or "d-needs": esteem, friendship and love, security, and physical needs. With the exception of the most fundamental (physiological) needs, if these "deficiency needs" are not met, the body gives no physical indication but the individual feels anxious and tense. Maslow's theory suggests that the most basic level of needs must be met before the individual will strongly desire (or focus motivation upon) the secondary or higher level needs.
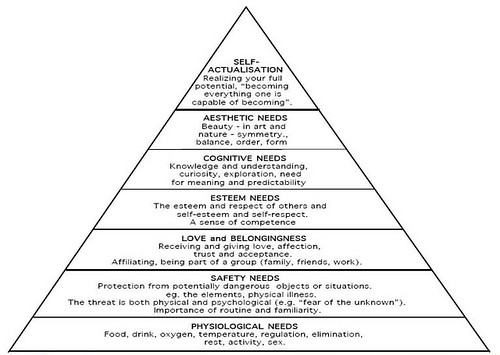
The people I work with are severely and chronically challenged to move beyond the second tier: Beyond oxygen, everything is a struggle for them.
The constant lack of any income other than their SSDI which is most sucked up on that outrageous rent causes and sustains major turbulence in getting food and rest. They may pay rent, they may have a room indoors and a bathroom to use but that is about it.
It doesn't help them through the second tier:
Safety and Security needs include:
Personal security
Financial security
Health and well being
Safety net against accidents/illness and their adverse impacts
They have no real security in these homes. They can't be protected much from theft or threats. No finances means no financial security. Health and well-being? These people have no access to healthcare. Usually when sent to the hospital it's for psychiatric reasons. Nursing assessments will be completed and problems documented but little gets done.
Yes, some folks do have Medicaid and ALL these people qualify for it, but once they go into a jail or a state hospital, that is cut off and it's a bitch to get re-started. And yes, people are discharged from jail and hospitals (state hospitals) without ANY effort to get this restarted.
So they get discharged - very often - either to a transitional home or to a community counseling program called Assertive Community Treatment which will assist them in finding one of these crappy places to live and will make some facsimile of an attempt to help these people work on stability.
However, I just got done with a long-winded description of how crappy these transitional homes are. They do NOT promote or provide the stability these people desperately need.
Without that most basic stability - living in a home for months on end, uninterrupted, not evicted, not jacked around - none of the efforts anybody expends does much good and they will continue to decompensate and they will continue to go in and out of hospitals and jails. You can bank on it.
I have witnessed this firsthand many times now. It's one major reason I am writing about this.
It doesn't have to be this way
Georgia settles suit on confinement of disabled people out:
The Justice Department deal is expected to serve as a model for enforcing rights of the mentally ill.
The agreement, announced Tuesday, resolves a Justice Department lawsuit brought in January under the Americans with Disabilities Act.
It also caps a federal investigation that began after more than 100 suspicious deaths of patients in state mental hospitals were documented over a five-year period in a 2007 series in the Atlanta Journal-Constitution.
The federal investigation confirmed an "alarming frequency" of preventable deaths, suicides and assaults in the hospitals.
So the stories my cliente tell me at the partial hospitalization program and often true and were happening just a couple of years ago, let alone 40 and 50 years ago.
Another perspective on what this means comes from Psychiatry Online
Federal Lawsuit Ends With Major MH Care Investment
Rich Daly
A statewide system of community-based treatments and support services for people with serious psychiatric illness in Georgia is expected to emerge from a final settlement of a lawsuit brought against the public mental health system by the Department of Justice.
Public mental health services in Georgia are expected to improve dramatically as a result of a wide-ranging settlement of a lawsuit against the state that has dragged on for years.
The lawsuit was initially intended to redress the harmful conditions of the state's psychiatric hospitals, but the settlement goes further: it requires the state to commit to a series of reforms in its public mental health system, including a large expansion of its community-based treatments and supports.
The government is forging ahead with plans to empty out the hospitals of all but the most dangerous and fragile and have everybody in the community.
Georgia is notoriously callous to the rights and needs of the mentally ill and MR/DD populations and it has taken an alliance of various professional groups and activists 10 years to twist Georgia's arm to do anything to protect these people from the things I have told you about. Fought it tooth and nail.
Much of the presentation one sees with the chronic, older population is largely a result of years of medical neglect and poverty. Once people were labled with "mental illness' their lives went off-track. Partly due to the ravage of mental illness and partly due to being discounted and shoved into warehouses and just not cared for properly, if not violated, abused and killed.
From the Psychiatry Online link:
Psychiatrists and other mental health advocates said that the agreement's most important benefit is that much of the estimated $130 million it requires the state to spend over five years on mental health services will fund an expansion in community treatment, including 24-hour community “crisis service centers,” psychiatric beds in private hospitals, psychiatric crisis-intervention teams, and other local services.
I have seen and worked for some of these community based teams: mainly assertive community treatment teams, and frankly, I ain't impressed with any of them.
I will assume there are some good ones but I am aware of several bad ones as evidenced by either working for them or noticing that they are forever trying to hire professionals like me to work there. They can't keep them usually because the conditions are brutal: Lots of driving, going into sketchy neighborhoods and chaotic group homes attempting to "do therapy".
The documentation standards, at least for Medicaid programs are simply unbearable. Despite it's ostensible goal of 'reducing fraud' and "ensuring best practices, it comes off like a way to get people treated for free in the community by ravaging the agencies with documentation audits that force huge paybacks to Medicaid.
There is almost no way to have a set week and time off, its' a 24-hour sort of thing and several of the agencies of which I am aware of often have 'issues' with paying staff on time or properly, also leading to attrition. In managed care if you can restrict the availability of providers you have cut costs.
This does not result in or reward quality (or even remotely effective) community care. It is an outrage; it is a tragedy of wasted money and wasting time and people's lives. It occurs because of ignorance, incompetence, from amateurs trying to do something they do not have the experience to do, and from fraud.
With the continued process of moving people with severe mental illness into the community these transitional homes should be - must be - banned. They need to be eliminated and replaced with licensed, regulated, and monitored homes that provide the sot of structure and care that they will need to live in the community without decompensating, being exploited for their check, confronted with serious crimes, or going missing.
There also needs to be consortium of sorts wherein one can find residents and homes without there being so much haphazard decision-making. I am aware of/have visited very nice and potentially very nice homes - available thanks to the demolished housing market - which need proper management (I can't believe I said that!) in order to pull this off.
There also needs to be a way to regulate or more consistently monitor the privately owned ACT treatment agencies to make sure that the treatment is really effective. This combined with proper residential experiences can help people solidify the base of their triangle and to begin thinking about what else they need to be doing with their lives.
In a properly managed system, people who have severely decompensated would be discharged to a proper licensed group home and an ACT team would provide the structure the person needs - managing to solidify the two lowest rungs on Maslow's triangle and decrease their risk for relapse.
PH programs, like the one I work for, serve as a way to provide sustained intensive psychiatric treatment and monitoring for persons who need a higher level of structure to prevent re-hospitalization but do not need to be in a locked facility 24 hours a day. The goal is to maximize stability and to discharge them to an ACT team for ongoing follow-up.
Of course some people need additional work on specific issues that can be addressed in other free-standing specialized groups (like AA or incest survivors) or with the establishment and maintenance of a relationship with a private therapist to work out long term solutions.
I believe it can be done, IF there is a desire to get it done.
We can pay for insane wars and give hundreds of billions of our tax dollars to the wealthy for no defensible reason, we can shave off some crumbs to help keep these people out of living in squalor while they try to get their lives together.
If nothing is done to regulate these outrageous transitional homes and amateur-hour ACT teams,more and more tragic stories like I have only hinted at in this article will escalate.

