No I’m not talking about the state of politics in America. I’m talking about our bodies. Modern molecular biology has taught us to think of our bodies as machines, astounding complex, amazing pieces of engineering. But there’s another way to look at it. Our bodies are a result (not the result or end product) of a few billion years of evolution. They are both amazing machines and a hodgepodge of historical accidents, compromises, and the current results of evolutionary warfare.
Medical science treats the body as a machine, like a particularly complex appliance with some ability to heal itself. Recently many researchers have attempted to bridge the gap between medical science and evolutionary biology. Evolutionary medicine is a new and exciting field.
My university hosted a symposium on Evolutionary Medicine this past Friday and Saturday. They have a very cool graphic which you can see here. My guess is that our governor probably wouldn’t be too happy about this on multiple levels. However it was funded by an endowment and no tax dollars were used. Unfortunately I was only able to attend a few sessions because of my other responsibilities and a rather selfish desire to get some exercise and enjoy the beautiful weather yesterday afternoon. But I’ll talk about a few of the topics at the meeting and a few of my own.
Age-Related Diseases – A century ago and through large portions of human history infectious diseases were probably the major cause of human mortality. Today, in the western world, various cancers and diseases of the circulatory system are what finish off most of us. Why did these diseases step up and ‘fill in the gap’?
Heart disease and cancer are mostly (although certainly not exclusively) diseases of individuals that are middle-aged or older. They are the result of the evolution of senescence. I have discussed this before in this diary. Let/s briefly review.
Senescence (the decline in physiological competence with age) is the best contradiction to the phrase ‘survival of the fittest’. Amoebae and bacteria are essentially immortal unless you regard splitting it two to form offspring as dying. Philosophically you could debate the point but biologically it is clear – nothing dies in that situation.
Furthermore although all organisms (as far as we know) that have a separate germ line (i.e. eggs and possibly sperm) show senescence they do so at staggeringly different rates. A fly is ancient in weeks, a bristlecone pine can live for millennia.
The solution is to understand how natural selection varies with age. Consider an animal species that is immortal in the sense that individuals will never die of old age but that can be killed by predators or accidents. The individuals of that species will have an average lifespan dictated by the frequency of deaths caused by outside forces. Some individuals will be lucky (or careful) and live many times that average lifespan but they will be few in number.
Now imagine that a mutation arises and spreads to a few individuals in the population. It is advantageous early in life but has bad effects at later ages. Because virtually individuals are alive at young ages (and produce most of the offspring) and very few individuals are alive at older ages the mutation is on average beneficial to individuals holding it and it will spread.
Populations with higher externally driven mortality will thus be under stronger selection at young ages and weaker at old ages and evolve a shorter lifespan. The reverse is true for populations with lower external sources of mortality. The diary cited above discusses the comparative data (i.e. lifespans of different animals) supporting this hypothesis.
Changes in tuberculosis infection over the 20th century. In the early 20th C most infected individuals are of reproductive age. There is strong selection for resistance to the disease. In late 20th C most individuals infected are post reproductive and selection will be weak.
Genomic biologists have studied the evolution of the molecules involved in the control of the cell cycle. The cell cycle is the reproductive cycle of cells. Many genes and gene products control this cycle – moving it forward or keeping it in place. Many of the ones that first appear in animal cells (as opposed to the cells of single-celled or colonial (colonies of cells) organisms) are ones that are often associated with cancer. Having a complex body with different organs and tissues requires much finer and more complex control of the cell cycle – more things that can go wrong. The advantages of a complex body apparently outweighed the costs of a risk of cancer or we wouldn’t be here.
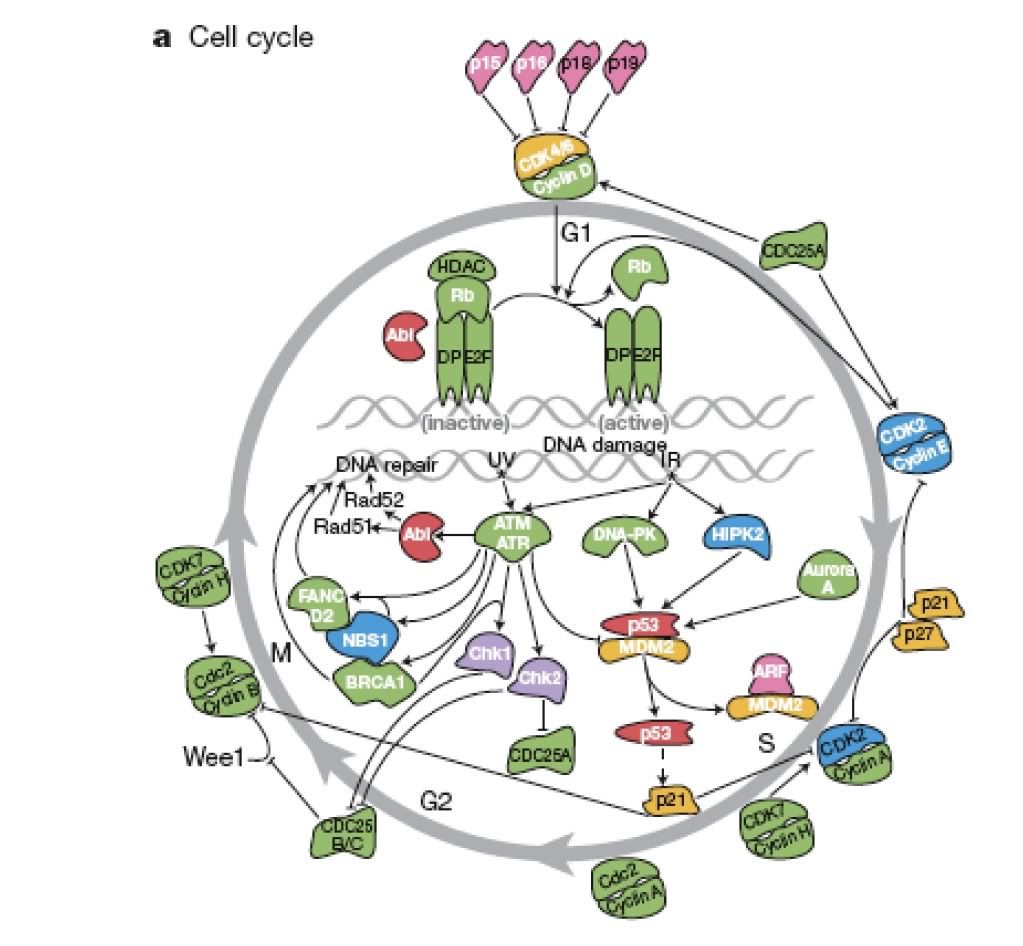
Genes controlling the cell cycle, ones in blue, orange or pink are ones that evolved in animals - many of these are implicated in cancer.
One of the speakers spoke on a topic with which I was unfamiliar, the endothelial system, the layer of cells lining the inner surface of our blood vessels. This layer is highly variable in structure, reflecting the different demands placed on it in different blood vessels. It is apparently unique to vertebrates and the speaker is studying the nature of the endothelium in hagfish, the earliest branch of living vertebrates. He thinks that perhaps the nature of the endothelium may predispose us towards heart disease.
Infectious Disease One of the more obvious aspects of evolutionary medicine is our interaction with other organisms (or quasi-organisms such as viruses) that make us sick. These entities evolve just like us, in fact they evolve much more rapidly than we do. Their tight associations with their hosts (i.e. us) and their extremely rapid generation times make them excellent examples of evolution.
Our treatment of infectious diseases depends, to a large extent on their evolutionary history. There is no cure for the common cold because the cold isn’t a single disease – it caused by a large number of closely related species. Gaining immunity to one doesn’t affect any of the others. Influenza is caused by a virus that evolves so rapidly (although the media calls it mutating, that is only the first step) that a new vaccine is needed annually. And diseases escaping into previously unexposed populations (either by leaping to a new species or invading a previously uninfected area) can have devastating consequences.
One potent link between medicine and evolution in this area is methodology. The history of a disease, its place of origin, and pattern of dispersal can be studied by reconstructing its phylogeny (evolutionary family tree). The medical researchers doing this are using exactly the same techniques an ornithologist would use to figure out the evolutionary relationships between species of owls although the time scale for the micro-organisms would be years or decades rather than millions of years. These techniques have allowed researchers to trace the origin of HIV in Africa for example.
Phylogeny of HIV showing multiple transfers from other primates to humans.
This evolutionary understanding of disease is immensely useful. Our lifestyle and medical practices are enormously beneficial to microbe evolution. We apply strong selection pressures through the use of drugs, we move around allowing infection of new populations, and we live in very densities (and keep domestic animals at even higher densities). This combination of strong selection, large population sizes, and high rates of movement is a recipe for rapid evolution. Hence the continued concern about outbreaks of new diseases.
The Microbiome A tree in the rainforest is an entire ecosystem. Epiphytic plants grow on its branches, trapping water and allowing animals to live in tiny aerial pools. Monkeys and sloths live in the branches along with countless insects eating fruits and leaves. Snakes snag passing birds. Mycorrhizal fungi live entwined with the roots in the soil. It has been estimated, for example, that a single tree in the Amazon may be home to more species of ants than are found in all of Great Britain.
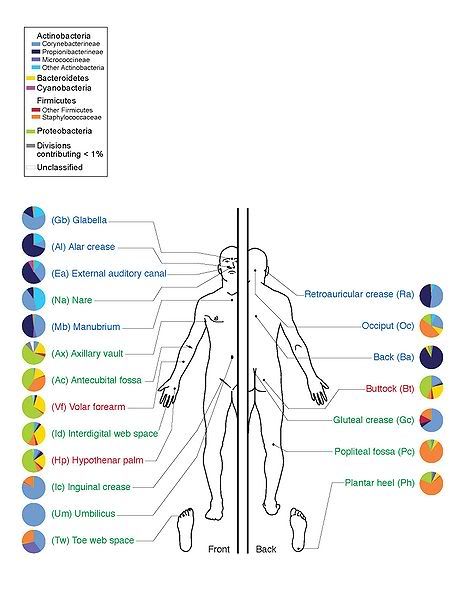
Similarly, although on a small physical scale, our bodies are home to countless other organisms. Bacteria in our guts, on our skin, virtually everywhere. Fungi, mites, and so on. We are walking ecosystems and these organisms have co-evolved with us. Their contributions to our health are barely understood.
Education and Practice There is apparently a push to emphasize basic science and the process of science more in medical training (as opposed to memorization of enormous amounts of factual information) and at least some people are interested in teaching medical students more about evolution. The obvious difficulty is the rather packed nature of the medical school curriculum. Another difficulty was pointed out by a speaker at the conference. His Dean had declined to add a course on evolutionary medicine to the med school curriculum saying he was ‘agnostic’ about evolution. My jaw dropped – a Dean of a Medical School said that – and it was not from a region of the country where you might suspect that.
One topic that comes up on dkos a lot is science and antiscience. Medicine and evolution is a wedge to insert a bit more science into everyone’s day to day existence.
