Donald G. McNeil of the New York Times reports the shocking news that three African governments have implemented a "cordon sanitaire," cordoning off a perimeter around an infected area allowing no one out of a widespread quarantined area. Other neighboring countries have closed borders and banned flights from some of the worst afflicted areas.
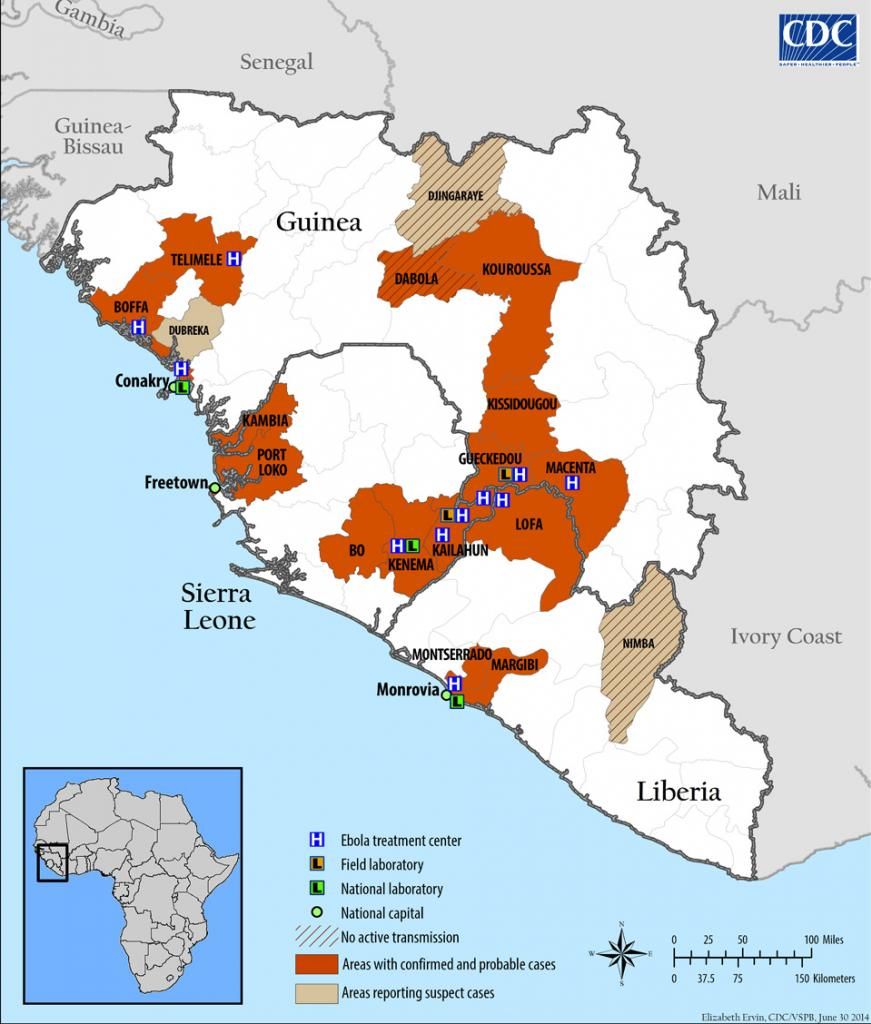
In, Using a Tactic Unseen in a Century, Countries Cordon Off Ebola-Racked Areas, we learn that health authorities consider an area the size of Jamaica, at the intersection of Liberia, Sierra Leone, and Guinea, to be a 'triangle of death', so dangerous, and out of control, that governments have positioning military troops last week to close roads and prevent anyone leaving the infected area. 70% of the Ebola cases so far have occurred in this region.
Even a month ago, Liberian government officials announced anyone hiding, or not reporting possibly infected family members, or others who show symptoms of Ebola could be subject to arrest.
The Ebola outbreak in West Africa is so out of control that governments there have revived a disease-fighting tactic not used in nearly a century: the “cordon sanitaire,” in which a line is drawn around the infected area and no one is allowed out.
Cordons, common in the medieval era of the Black Death, have not been seen since the border between Poland and Russia was closed in 1918 to stop typhus from spreading west. They have the potential to become brutal and inhumane. Centuries ago, in their most extreme form, everyone within the boundaries was left to die or survive, until the outbreak ended.
Plans for the new cordon were announced on Aug. 1 at an emergency meeting in Conakry, Guinea, of the Mano River Union, a regional association of Guinea, Sierra Leone and Liberia, the three countries hardest hit by Ebola, according to Agence France-Presse. The plan was to isolate a triangular area where the three countries meet, separated only by porous borders, and where 70 percent of the cases known at that time had been found.

The outbreak started in southern Guinea in December, or perhaps earlier last year, and was first detected in late February of this year. Since March I've written over two dozen articles about it, however, I have been moving from Massachusetts to Florida for the last two weeks, and without internet, so missed reporting several important major milestones, such as the total death count passing 1,013 with 1,848 total reported cases, which is almost certainly a significant under count as health authorities can not get to many remote regions, and villagers are now so hostile to health authorities they will not allow them into many remote regions under the false impression that it is the health authorities spreading the disease.
An official from the Center of Disease Control and Prevention expressed support for the tactic but also is concerned that the implementation be as ethical and as humane as possible to minimize starvation, lack of water, and other impacts of people trapped withing the quarantined area. Ways must be found to get food, water, and medical care into the devastated region where Ebola is raging out of control, until it "burns itself out."
“It might work,” said Dr. Martin S. Cetron, the disease center’s chief quarantine expert. “But it has a lot of potential to go poorly if it’s not done with an ethical approach. Just letting the disease burn out and considering that the price of controlling it — we don’t live in that era anymore. And as soon as cases are under control, one should dial back the restrictions.”
McNeil reports that in Sierra Leone an area the size of Jamaica, in the Kailahun and Kenema districts, has been cut off my military roadblocks, although some passage is being allowed with proper credentials and medical checks including temperature.
Since I last reported, several weeks ago, 10 cases have developed in Nigeria, the forth country to report cases. All of these cases were related to a Liberian American who arrived on a flight from Liberia and collapsed in the Lagos airport. Nigerians are reported to be furious that he was allowed to fly to Lagos after his sister died of Ebola.
Reports from inside the quarantined areas in Sierra Leone and Liberia indicate trapped citizens are terrified, not just of catching Ebola, but also of starving, economic collapse, and lack of water, as much of the income in these areas comes from trade, including game meat which is now banned.
We can only imagine that cordoning off vast regions with military troops, and having the Liberian government threatening to arrest anyone not reporting family members, or hiding them if they have flu-like symptoms, will "complicate" efforts to gain public "trust."
No specific plans for delivering food, water, or medical care to these regions has been announced, although the World Health Organization has declared it plans to attend to such matters as some point.
Doctors Without Borders, aka MSF, has been vindicated, in my opinion, in its long running feud with the WHO, who it claimed was downplaying the extent of the outbreak for political reasons.
Readers here may remember several articles I wrote over a month ago reporting the Director of MSF to be the first expert to declare the "outbreak" out of control, and that MSF no longer was able to send teams to areas reporting new outbreaks. He received much criticism from officials from the WHO who reassured everyone at nearly every announcement that the outbreak was under control, and implied MSF was being alarmist.
MSF and WHO have been at odds since the very first week of the announcement of the first detected cases when the WHO criticized MSF for reporting an "Ebola epidemic" while the WHO insisted media report it as an "Ebola outbreak" as I have here after "correcting" my first articles here where I followed the first MSF reports. MSF was also the first to declare this "outbreak" unprecedented, especially calling attention to the never before seen degree of multiple epicenters of outbreak, which have made this outbreak so unusually difficult, or should we say, "as yet impossible to contain."
Please allow me a few hours today to reestablish my computer set up and bring you up to date on numerous other dire and sad Ebola related Stories, and outbreak maps. Sadly, after reporting the death of heroic Dr. Khan, several weeks ago, another doctor, and dozens of additional health workers have died, or become infected in these last few weeks, leading to even greater shortages of health personal, as even many who have been courageously serving since March, are now fearful of continuing to treat infected patients, or entering infected areas to do contact tracing which exposes them to many risks even when taking all the recommended precautions.
From what I can gather from a few other reports, this cordoned of area may be considered too dangerous for even protected health care workers to enter, which may have been one factor leading authorities to be appearing "to be giving up on the region" in a massive geographical triage, unprecedented in the last century. I need to do more research which I will include in updates.
Another comment I would like to add, to illicit discussion from some of our mathematical and epidemiological experts relates to the unusually "low" reported morbidity rate of "only" 60% in this outbreak compared to 90% in prior outbreaks of the Zaire strain of Ebola.
Last month just before shifting to moving mode I informally estimated that based on the evidence so far, the exponentially growing infection seemed to have a "doubling time" of just over a month based on a "positive feedback loop," meaning "reinforcing" not "good," where the number of contacts between the "Infected Population," and "Non-infected Population" create the rate of "New Infections." After an incubation delay of 2 to 21 days, symptoms emerge, with death occurring in over 60% to cases in the following week, and 90% of cases in prior outbreak of the Zaire strain.

Although this outbreak is still described as the Zaire strain, initial genetic analysis indicates it is 3% different, meaning that what I predict will eventually be named as a new Guinea strain, diverged from the Central African strain long, long ago, perhaps, even hundreds of years ago, and has only been noticed now. Previously, outbreaks of Ebola are thought to have come and gone unnoticed, because they would essentially totally wipe out remote afflicted villages, and then lurking unnoticed in the reservoir species of fruit bats.
A deadly combination of extensive deforestation, and greater population mobility is though to have not only brought about greater interaction infected fruit bats and people, but also enabled infected people to travel more widely before being noticed.
So far discussions of the mystery of why the mortality rate of this outbreak is so much lower than the 90% death rate usually associated with the Zaire strain has failed to include the straight-forward mathematical observation that in an outbreak growing so fast and the countable deaths occurring up to a month after infections we should expect to see the observed death rate be a lower percentage than previous outbreaks that are over, due to what is called "steady state delay." If we just used the death count to the known cases, we should expect a "bias" due to the continuous stream of new cases will make the death ration appear to be lower because of the delay in actual deaths. I have not yet been able to analyze enough raw data to determine if these mathematical aspects of information delays have been properly considered.
We do know that those afflicted who report early and receive proper hydration, antibiotics to control secondary infections, and other top level, early medical attention have a better chance of survival. Later I will update this report with article describing a new medication called Zmap, and even promising new possible vaccines.
As always, let me express on behalf of the Daily Kos community or prayers and best wishes for recovery to all those afflicted, and sympathy or the families, loved, ones, and all Western Africans during this horrible situation. Please know that we have been concerned about your plight from the first report in late February and early March and many here are working on ways we may be able to help, beyond merely reporting on this dire "outbreak" from the very beginning.
9:41 AM PT: