The term narcotic is actually pretty archaic, since many drugs that are not narcotics have traditionally been lumped in with the true narcotics, but it is a term that people recognize. A better term is opiate, which nails it down in a more precise fashion.
I will adhere to the latter convention, because the term "narcotic" has been associated with cocaine, certainly not a narcotic, to Cannabis, also certainly not a narcotic, to several others. In the old legalese, anything that was not alcohol and a drug was likely to be called a narcotic.
First, a little housekeeping. First of all, I still have not bought cigarettes since March. I am still rolling Prince Albert, but have started tapering off. Second, my fingers are just about well now. Here is a picture (the last one) of them today, four weeks and one day after the burn:

Almost all modern opiates derive from the opium poppy, Papaver somniferum, except for the synthetics that mimic the pharmacological actions of the alkaloids contained therein. This plant, native to Eurasia, is cultivated worldwide both for culinary purposes (the seeds) and the resin (crude opium) that it produces in defense of scaring of the seed pod when it is green and the seeds are still developing.
Here are a few pictures. The first one is of a typical poppy field, and the second one of a poppy seed capsule bleeding out alkaloid rich latex, which is sort of like our blood in that it clots and begins to heal the wound. The color of the flowers is quite variable, and red, white, and purple are quite common, along with variegated ones like the one shown.


As shown, when injured, the seed capsule of the opium poppy exudes a healing latex in defense of the injury. Interestingly, if the injury penetrates completely into the ovary, the capsule usually just withers and dies, producing no salable opium. Folks who raise them for a living know to penetrate the surface very lightly. There are also differences in different cultures, some making the illustrated vertical cut, and others making horizontal cuts.
In any event, after the latex exudes it is allowed to dry somewhat and the workers come back in a day or two and scrape it off and collect the scrapings. If the pod is immature enough, they will scarify it again and repeat the process until it gets too woody to exude latex. Then they are allowed to ripen for poppy seeds and next year's planting.
Depending on the final intention, the gum is either dried further (often under wood or poppy straw smoke) or taken to extraction. The former process produces gum opium, the legal (and illegal) starting material for many narcotics, including the opium of trade itself. For illegal heroin production, good quality gum opium is not that necessary, just the chemicals in it. Obviously, drying out some of the water makes it easier to transport.
Opium contains dozens of alkaloids, many of which are pharmacologically active. The most important one is morphine, and the United States Pharmacopoeia has strict limits as to the morphine content. Interestingly, this compound is named after the Greed god Morpheus, the god of sleep. There are many minor alkaloids, amongst them papaverine, which has completely different actions that are also useful as medications.
Other than producing pharmaceutical morphine, gum opium has a shrinking market. It is heavy and bulky, and has a characteristic odor that is easy to detect. Whilst it is used illegally still, there is not much of it on the illicit market.
In the old days of the United States, opium was easy to find. Before the Harrison Narcotic Act of 1917, anyone could go to just about any pharmacy and buy morphine, heroin, paregoric, and laudanum. The latter two were solutions of opium in strong alcohol, with paregoric having camphor added to it. These two last preparations were often used to quiet "colicy" infants, and that was a really bad idea. They were also rubbed on the gums for teething crying. Opiates have little local action, so most of the action was systemic. They just went to sleep.
After the Harrison Act, access to opiates became much more restricted. Still available by prescription, the number of physicians prescribing then declined dramatically, because in the 1930s the notorious Harry O. Anslinger, head of the Bureau of Narcotics and Dangerous Drugs (BNDD), decided that most people should not have access to them. Anslinger also was the driving force, along with William Randolph Hearst, to make Cannabis illegal. He once boasted that no matter what laws were changed by the states or the Federal government, Cannabis would always be illegal because he saw to it that an international treaty was ratified outlawing it. Thanks, Harry.
Well, coincidental to, or almost so, to the Harrison Act was the 19th Amendment, making beverage alcohol illegal in the United States. Yes, THIS United States. All of a sudden, beer, wine, and liquor were ILLEGAL for everyone. I know that no one reading this remembers, since it happened the year that my dad was born, in 1919. But it became the law of the land. Suddenly, a social event, having drinks with friends and family, was ILLEGAL! Well, there was lots of public demand for liquor and many folks ready to take the risk to supply it. This is the genesis of the Mafia in the United States, and the ratification of that amendment has consequences still today. Woodrow Wilson, the very vacuous, idealistic Democratic president signed the bill, and the States ratified it. Talk about unintended intentions!
The mob started distributing a product that the People wanted. This I find disturbing in many ways. First, silent civil disobedience is not civil disobedience. It is outlaw, and I will further state that Cannabis users are silent for the most part, just hovering beneath the law. Change the law! Do not just meekly break it, but that is my editorial comment.
Second, the mob made a fortune out of it because the former excise taxes that had gone the the government now went to the mob. As they got rich, they refined their smuggling channels for a very heavy, bulky product. Third, the law enforcement infrastructure became co opted, if not completely corrupted.
Then Franklin Roosevelt was elected to office. The mood of the Nation was changing, and the amendment to repeal Prohibition was passed. Roosevelt signed the bill, and the States ratified the amendment in December of 1933. But the damage was done. The mob had been anticipating this for several years, and started substituting narcotics, particularly heroin, for alcohol several years before.
Whilst I am not a smuggler, I am a bona fide scientist, and understand a fair amount of economics. If I had a product with a huge illegal market that was going to be made legal, I would want to get into something more lucrative. If I were already transitioning to heroin, I would try to make it cheap and addict as many people as possible. Then, when alcohol became legal again, I would have a new market. This is exactly what happened. Also, an alcoholic in the prime of her or his addiction will consume half a kilogram or so a day, whilst a heroin addict, in her or his prime, will consume maybe a few milligrams a day.
Think about this. The same boat that took cases of booze that folks wanted could now take thousands of doses that folks needed. And as the risk went up, the profit did as well. That is the situation that we have now. Poor decisions made almost a century ago still haunt us. The lesson here is that we need to make better decisions, like taking all Cannabis laws off the books. But that is another editorial comment.
Now the the physiology of opiates. As you know, from reading my posts in this series for a long time, there must be a nervous system receptor for opiates. For simplicity, we will assume morphine as the agent. It gets complicated. I need to explain the agonist versus antagonist model.
A pure agonist binds with a particular receptor and potentiates the effect of that receptor. A pure antagonist binds to the same receptor, but blocks the effect of the agonist. Most opiates are mixed, with both agonist and antigonist effects. Morphine is pretty much a pure agonist. Heroin is morphine on steroids. The antidotes to opiates are predominately antagonists.
Now we have to get wankish. As of this writing, there seem to be at least four types of opiate receptors in the human brain, and many subtypes of the four. I suspect that there are many more that are yet undiscovered.
The delta ones are involved, but do not seem to be the largest contributor to analgesia. They might have a weak contribution to respiratory depression but do not seen to be the largest contributors. No doubt they are important and we just do not understand everything yet.
The kappa ones are not well understood, but I think that they are important. Conventional wisdom says that stimulation of them makes you feel bad, or paranoid, but there is much more science to be done. At least three subreceptors have been identified, and I am not convinced that we know as much as we need to know.
By far the most important, as our science can tell us, are the mu receptors. They are the ones that respond the most to morphine, and indeed, the Greek letter mu was chosen for morphine, with the initial letter "m". No one knows how many subtypes exist for them, but they are all over the place in the body. It is the interaction with opiates with the mu receptors that cause the deleterious effects of opiates.
For example, many of these receptors exist in the brain stem, which regulates breathing. Most heroin overdose patients die from respiratory collapse. There is another subset that in common in the large intestine. That is why heroin makes you stop defecating, and that designer drugs like the over the counter remedy Loperamide, also called Imodium.
Morphine is the prototypical opiate. It is extensively used an a potent analgesic, especially in hospital settings. It is not used as often in home settings, except for terminal patients, because it is highly addictive and a fairly potent respiratory depressant. Other drugs are used for home settings, including codeine (also often used for cough), hydrocodone, (Vicodin) (also used for cough), hydromorphone, and the much celebrated oxycodone (Percodan and the notorius OxyContin). These are listed roughly in order of increasing potency. These drugs range from Schedule V in the Controlled Substances Act to Schedule II, depending on dosage and what other drugs are in the particular preparation. For example, codeine containing cough syurp is often Schedule V, while oxycodone products are Schedule II.
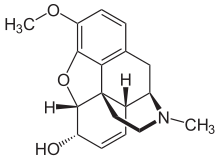
There are many other "natural" opiates on the market. These are just a few for illustration. I use the term natural to denote that they are all based on the basic structural skeleton found in morphine and codeine, two alkaloids present in opium. The others are semi synthetic is that some of the "chicken fat" (a very technical term that we organic chemists like to use) hanging off of the basic molecule. Here are some structural formulae:

Morphine
Codeine
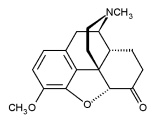
Hydrocodone
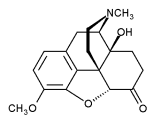
Oxycodone
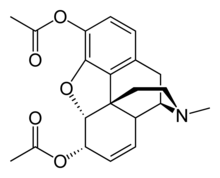
Heroin
The most notorious opiate is diacetylmorphine (heroin). Because of the two acetyl groups, it is much more lipid soluble than morphine, and so crosses the blood brain barrier more easily. Heroin is a Schedule I drug in the United States, meaning that there is no recognized medical purpose and so the material is illegal in all situations except for specifically licensed studies approved by the Drug Enforcement Administration (DEA). Potent and (relatively) cheap, heroin is highly addicting and very recovery from it is very difficult.
UPDATE: I meant to give a brief history of heroin, but I was having HTML trouble with the pictures. So here it is now. Heroin was developed in Germany in the late 19th century as a "nonaddictive" alternative to morphine. Yes, you read that right. It was found that by manipulating the chicken fat around morphine, a drug with similar properties but much more potent resulted, and they named it heroin because they thought it would the the hero to save people from opiate addiction whilst still giving the positive effects. That was because, at the time, neurotransmitters and receptors were not understood, and pharmacology was in its infancy. They thought that because the dosage was so much lower for the same effect that addiction would be a remote possibility. We know better now, but at the time heroin was available in cough syrup (it is an excellent antitussive), elixirs, and about everything else. Now we understand that this was a foolishly naive take on things, but that was the thought. By the way, the reason that heroin is so potent is that the chicken fat allows it to pass the blood brain barrier much more efficiently than morphine does. In the brain, it is converted to morphine, so my epitaph "morphine on steroids". Ohhhhh, another topic for this subseries. Steroids are certainly drugs of abuse.
There are other classes of opiates, the fully synthetic ones. These are based on molecular skeletons other than those of the natural ones, but they work about the same way. A very commonly encountered one is propoxyphene (Darvon). The days of this drug may be numbered in the United States, as an Food and Drug Administration (FDA) panel has recommended that it be withdrawn from the market. Right now, it is Schedule IV, but it is not a very good analgesic and has a bad reputation for being involved in drug deaths. In combination with acetaminophen it is known as Darvocet, and this is particularly dangerous drug, especially for recreational use. Such use usually involved large doses, and acetaminophen is a known liver toxin in high doses. As a matter of fact, I was commenting on a health diary on Thursday about the dangers of this drug, and darned if FDA did not come out with a new warning about liver damage and it that I heard about on Saturday.
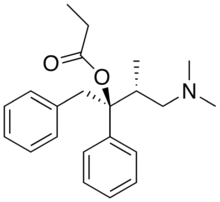
Propoxyphene
Perhaps the most well known synthetic opiate is methadone, also called Dolophine. It is an excellent analgesic, and is cheap. Thus, it is seeing increased use for chronic pain control. It seems to have a particular affinity towards the mu receptors in the brain stem, with the possibility of respiratory depression in relatively low doses. It is Schedule II.
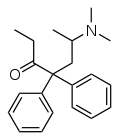
Methadone
The most famous use of methadone is heroin withdrawal. Methadone is long acting and prevents physical withdrawal symptoms in addicts. In higher doses, it also blocks some of the euphoric effects of heroin. This seems to be an effective way to help some addicts recover, but is not sufficient by itself.
A very common synthetic used widely in the past is meperidine (Demerol). It is still used, but not nearly as much as in the past. It is fairly short acting, so has to be given more often than, say, morphine, and has some unique toxicological properties, causing it to fall out of favor.
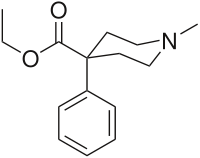
Meperidine
Another class of opiates are the fentanyls (there are several variations, depending on the chicken fat). They are extraordinarily potent, scores of times more than morphine for pain control, and are short acting. Thus, they are very useful in surgical settings, since the drugs wear off rapidly after administration ceases. I myself was given alfentanyl for surgery on my sinuses, and I promise you that I did not feed a thing. The fentanyls are often used as heroin or oxycodone substitutes or even passed off for the real thing. One common name for those is China White.
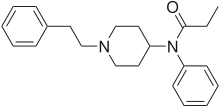
Fentanyl
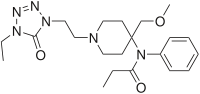
Alfentanyl
Alpha methylfentanyl
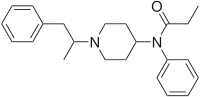
Another opiate worth note is 1 methyl 4 phenyl 4 propionoxypiperidine (MPPP) that is Schedule I but fairly easy to synthesize and so is used as a heroin adulterant or substitute. It is not unusual for unscrupulous people to create designer drugs to try to avoid the drugs laws, but this case is unique. By the way, you can see from the structural formulae that is is very similar to meperidine. Now, here is the wild part. Because of the process used to produce MPPP the first time for illicit use, a major impurity called 1 methyl 4 phenyl 1,2,3,6 tetrahydropyridine (MPTP). It turns out that MPTP is rapidly metabolized to a very active ionic species that specifically attacks the dopamine producing cells in the part of the brain responsible for voluntary movement, killing them. The result is severe Parkinson's Disease, developing in the matter of a few weeks, depending on how much of the contaminated drug was used. Some of the addicts continued to shoot up until they literally could no longer move to fill their syringe. There is no recovery from that. The thing is that they knew that they were getting more and more motion impairment every time they shot up, but still did not stop.

MPPP
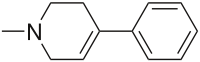
MPTP
I could go on much further, but I think that the points are made. There are literally hundreds of opiate drugs, and many of them are used in medicine to the great benefit of humanity. Unfortunately, these drugs have also been used for recreation, and that is a dangerous practice. In addition to physical and psychological addiction, several toxic conditions are associated with opiate overuse. One such condition is hearing loss. I have a relative who has been prescribed heavy doses of opiates for severe pain, and he is all but deaf now. There is also a rather controversial radio talk show host who lost his hearing as well, but had the resources for cochlear implants to help his condition.
Well, you have done it again: wasted a perfectly good batch of electrons reading this poor excuse for a post. And Rush Limbaugh considers changing to a progressive talk show host when he reads me saying this, I always learn much more that I could possibly teach writing these posts, so keep those questions, comments, tips, recs, and clarifications coming. Next time we will start the multipart series on psychedelic drugs.
I am also soliciting ideas for future series. I got some quite good suggestions last week, and in a week or two will pull the best ones for a poll, so suggest away.
Last Update: thanks to your valued readers, this poor work came in at number 39 on the jotter High Impact Diaries list just issued. The tips help, and so the the comments. But the list is driven by the number of recommendations. I very humbly express my appreciation to the community for the support. One of you even emailed me and we had a long telephone conversation. I feel honored. This is not very usual for a scientific diary as opposed to a political one, and I thank every one of you.
Warmest regards,
Doc
