At Netroots Nation, I was fortunate enough to participate in a science panel moderated by Mark Sumner and featuring Naomi Oreskes and Erik Conway (Merchants of Doubt), and Josh Roseneau (National Center for Science Education.) Their pieces can be found here, here, and here in the order they were given and are well worth the time to view.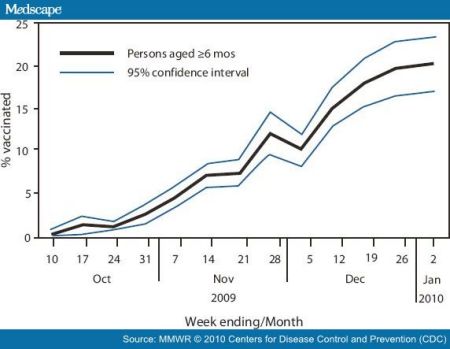
For my part, I had a piece about pandemics and vaccination, noting that one of the interesting effects of having a non-seasonal flu H1N1 influenza pandemic was the result of people being more willing to get a non-H1N1 seasonal flu vaccine. It's important to review this topic; like the engineers reviewing the management failure that happened in the Gulf, it's the only way to make use of the lessons learned.
Still, there was reasonable success in vaccinating people, especially high risk groups. The Northeast was especially good about it, due primarily to the strategy of using schools to vaccinate children. The Southeast wasn't so good, and had small late outbreaks of pandemic flu relative to the rest of the country.
Why would people choose to get seasonal flu shots when there was a nonmatching viral outbreak? One reason was that seasonal flu vaccine was readily available in October while pandemic vaccine was not, and seasonal vaccine was also recommended. Another, however, is that pandemic vaccine was "new" and seasonal flu was perceived as being "old" and therefore more trustworthy (unpublished observations from patient discussion and conversation with colleagues as well as on line comments.)
This was a false concept. Essentially, every year the old flu strains taken out of the flu vaccine and this year's recommended batch is inserted. The only reason H1N1 pandemic strain was not in the seasonal flu vaccine was that it takes six months to manufacture the year's supply, and that usually starts around February. Unfortunately, the pandemic H1N1 strain appeared in late April and missed the deadline for addition to the regular seasonal vaccine, which had already started the manufacturing process. Six months later, the pandemic vaccine started to be shipped, and demand peaked in Nov-Dec. By that time, it became clear that this pandemic was of the milder variety (a bit of an oxymoron to say 'mild pandemic'), and demand dropped sharply. Had vaccine been available earlier, more people would likely have been vaccinated, but that alone would not have eliminated anti-vaccine sentiment. 
In terms of vaccine in general, the anti-vaccine message was consistent from celebrities. Bill Maher and Glenn Beck were two oft-cited examples, suggesting this was not a left-right issue. That has consequences, and we're seeing it now in the pertussis (whooping cough) outbreak in California.
In fact, this is a graph of pertussis cases throughout the country and over to the right, you can see the spike in 2004.
Is this an "access to resources" problem, something that health reform would fix? It isn't just a question of insurance and access; in an excellent piece, Christina Jewett at California watch notes that:
Seven of the 12 California counties with the highest whooping cough rates also have above average rates of kindergarten students showing up to school with "personal-belief" vaccine waivers, a California Watch review of state data shows.
and speculates that when upper income families eschew vaccine, lower income families pay for it through lack of access. In any case, what's resulted is the worst whooping cough outbreak in 50 years and six infant deaths. That last stat is prompting public health officials to recommend vaccination to pregnant women and those who are exposing infants (when adults get pertussis it is an annoying cough; when infants get it, it can be life threatening.) 
I love the title of Oreskes and Conway's book, Merchants of Doubt, because when it comes to vaccines, I know the doubters will be out in full force. So let's be clear: it is settled science that vaccines don't cause autism, there is no thimerosal or mercury in pertussis vaccine, it's not a 'new' vaccine, and the vaccine is needed.
Will that make a difference? To some, no (even medical personnel, including nurses and doctors who should know better, are pretty bad about getting their flu shots. The average immunization rate in a non-pandemic year hovers around 50%, which is disgraceful. This year, we got that up to 61% for seasonal flu but only 37% for pandemic vaccine.) Alas, whether it's this year's pertussis outbreak or next year's flu season, the rest of us will get exposed because of vaccination resistance. More from California watch:
Researchers took a global look at how personal-belief waivers drive whooping cough in a 2006 article in the Journal of the American Medical Association. They found that states – like California – that have easy-to-obtain-vaccine waivers saw a 90 percent higher incidence of whooping cough than other states.
That's a legislative issue that kids are dying for California to address.
