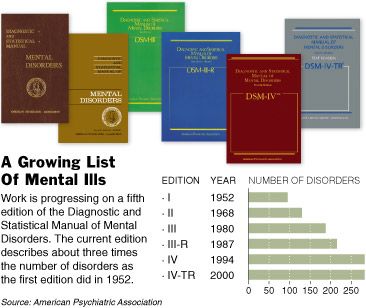
Yesterday, the board of trustees of the American Psychiatric Association approved the new DSM-5, aka Diagnostic and Statistical Manual, the controversial compendium of official definitions of "what constellations of symptoms doctors recognize as mental disorders," and diagnostic labels and categories insurance companies use to determine payments for services for mental illness. The new volume will be published in May of 2013.
In DSM-5: Psychiatrists OK Vast Changes To Diagnosis Manual, Lindsey Tanner describes three of the more controversial changes; dropping Asperger's disorder which is now included in "autism spectrum disorder, a new disruptive mood dysregulation disorder, and changing "gender identify disorder," now labeled as a mental illness, to "gender dysphoria," a condition of unhappiness about one's physically manifested gender."
The new manual adds the term "autism spectrum disorder," which already is used by many experts in the field. Asperger's disorder will be dropped and incorporated under that umbrella diagnosis. The new category will include kids with severe autism, who often don't talk or interact, as well as those with milder forms. ...
A new diagnosis for severe recurrent temper tantrums – disruptive mood dysregulation disorder. Critics say it will medicalize kids' who have normal tantrums. Supporters say it will address concerns about too many kids being misdiagnosed with bipolar disorder and treated with powerful psychiatric drugs. Bipolar disorder involves sharp mood swings and affected children are sometimes very irritable or have explosive tantrums. ...
Eliminating the term "gender identity disorder." It has been used for children or adults who strongly believe that they were born the wrong gender. But many activists believe the condition isn't a disorder and say calling it one is stigmatizing. The term would be replaced with "gender dysphoria," which means emotional distress over one's gender. Supporters equated the change with removing homosexuality as a mental illness in the diagnostic manual, which happened decades ago.
Below the squiggle I offer a more detailed description of the new DSM-V, from Science Decoded, and more extensive detail and some of the major criticisms of the whole methodology from Wikipedia.
_
In Diagnostic and Statistical Manual V: Small Changes with Big Implications Gina Putt, of Science Decoded, offers us more insights into the changes in the new DSM-V, with a view of how if affects women and other "kinder and gentler" changes, "such as the elimination of 'mentall retardation' in favor of 'intellectual developmental disorder.'"
According to Recovery Today Online, one major anticipated change in the new DSM-V will eliminate the category of “substance abuse and dependence” and replace it with “addictions and related disorders.” While the difference may seem semantic, the intent is to clarify that withdrawal is a normal response to the discontinuance of some medications, “whereas addiction is compulsive-drug seeking behavior.” The emphasis would now be on the behavior, rather than the physical response. ...
Gender Identity Disorder to Become Gender Dysphoria?
In what could be seen as a political move, the DSM-V is expected to focus more on the unhappiness that gender identity problems may cause rather than the issue of gender identity itself. Everyday Health notes that it is problematic if psychiatry ”casts one’s identity as an illness.” Focusing on emotional, rather than a state of being, appears to address this issue. ...
Some of the proposed changes have a disproportionate impact on women. Men would be unlikely to be diagnosed with the newly proposed “premenstrual dysphoric disorder.” As with gender dysphoria, the intent appears to be to focus on the emotions associated with PMS rather than menstruation itself.
Proposed upgrades to the personality disorders category are heartening. Women were frequently diagnosed as “histrionic” a personality disorder that is slated for deletion. The “disorder” included many criteria such as shallow relationships, focus on self, over dramatization and seductiveness. ...
Hoarding and binge eating have been on the scene for a while. Originally considered a type of OCD (obsessive-compulsive disorder) hoarding is understood to have distinct features. Binge eating, once only in the appendix of the DSM-IV will most likely be added to same category as anorexia. Children will no longer be bi-polar, but could instead be categorized as having “disruptive mood regulation disorder” to distinguish their issues from adult bi-polar disorder, which may keep children from being mislabeled and potentially, inappropriately medicated.
No discussion of the DSM-5 would be complete without noting some of the controversies and criticism of the entire approach, misuse of the categories, and methodological challenges, for which I draw from Wikipedia's excellent entry for DSM-V.
The British Psychological Society in the United Kingdom stated in its June 2011 response that it had "more concerns than plaudits".[59] It criticized proposed diagnoses as "clearly based largely on social norms, with 'symptoms' that all rely on subjective judgements... not value-free, but rather reflect[ing] current normative social expectations", noting doubts over the reliability, validity, and value of existing criteria, that personality disorders were not normed on the general population, and that "not otherwise specified" categories covered a "huge" 30% of all personality disorders.
It also expressed a major concern that "clients and the general public are negatively affected by the continued and continuous medicalisation of their natural and normal responses to their experiences... which demand helping responses, but which do not reflect illnesses so much as normal individual variation".
The Society suggested as its primary specific recommendation, a change from using "diagnostic frameworks" to a description based on an individual's specific experienced problems, and that mental disorders are better explored as part of a spectrum shared with normality:
[We recommend] a revision of the way mental distress is thought about, starting with recognition of the overwhelming evidence that it is on a spectrum with 'normal' experience, and that psychosocial factors such as poverty, unemployment and trauma are the most strongly-evidenced causal factors. Rather than applying preordained diagnostic categories to clinical populations, we believe that any classification system should begin from the bottom up – starting with specific experiences, problems or 'symptoms' or 'complaints'...... We would like to see the base unit of measurement as specific problems (e.g. hearing voices, feelings of anxiety etc)? These would be more helpful too in terms of epidemiology.
Overall, my first impression is that these changes represent improvements especially with regard to greater sensitivity to the language used that in the previous versions unnecessary stigmatized those with conditions that may be useful to diagnose for insurance purposes, but which should not be labelled cruelly, or pejoratively as mental illness.
Also, I haven't had time yet to study why the proposed "internet addiction," and "compulsive Daily Kos posting disorder, CDKPD," were not included, but I guess I should consider myself lucky not to have even more diagnostic labels than I already do.
Since my name as somehow been on the top of the "most frequent posters of the month" list now for almost two weeks even after Markos posted 70 in the election week alone, and I took off a whole week for Thanksgiving, I'm getting a little worried. Maybe this is another broken listing like the broken comment rating and Mojo counters which have been broken for over a year and a half? Because I've cut way back on posting. Really I have! I'm only an occasional "social" poster, now. But, my friends keep sending me literature on these 12-step programs for blogging addicts.

